The following text is a transcript from the course titled Making Sense of Meltdowns: How to Identify and Intervene For Children with Sensory Based Disruptive Behaviors by Nicole Quint, Dr.OT, OTR/L. We recommend following along with course handout to ensure understanding of the material.
Learner Outcomes
- The participant will be able to differentiate between behavior and sensory-based behaviors in relation to meltdowns in children.
- The participant will be able to identify at least 2 ways to determine if a child is having a sensory-based meltdown.
- The participant will be able to delineate at least four approaches to intervention for children with sensory-based meltdowns, including 1) reframe the behavior; 2) collaborate to prescribe sensory strategies to maintain arousal level for learning; 3) improve coping abilities with sensory strategies, and 4) environmental adaptation.
- The participant will be able to identify at least two ways to utilize sensory modulation strategies to prevent or reduce episodes.
Why Address Meltdowns as Pediatric Therapists?
Meltdowns and behavioral disrupt participation and/or performance occupations such as education, your play, your social participation, your self-care, and your sleep. It significantly can affect social interactions and communication abilities. It creates social and emotional distress for the child and the family. It can impact your development. If you're dealing with this as a child, it has consequences. Functional behavior plans do not work for this situation so this can lead to conflict in the exceptional student education (ESE) process. As soon as there's this additional layer of significant behaviors, things get a little bit more intense and I really think a lot of it has to do with role competence. People just don't know what to do in this situation and we're all professionals and when we don't know what to do, it can cause us to go into sort of an emotional pattern and when that happens, conflict typically ensues. Children with Sensory Processing Disorder and autism have disrupted white matter (that's been proven) and the tracts associated with social emotional processing is significantly affected for ASD, so we know that meltdowns are going to happen within that population. We also know it's going to happen within the SPD population because it's typically sensory-related. It is very interesting how it's there for both conditions but it sort of manifests differently. The other thing is it addresses family-centered care and that's always going to be a goal of in the pediatric environment and the adult environment. It impedes the transition process. Lastly and this is is so important, is that we can affect life-altering change and it's really not that difficult and that's the good thing.
Tool: Maslow's Hierarchy of Needs
When children who are either sensory avoiding or sensory sensitive they have a system that does not tolerate sensation well. The sensations are noxious to them and they can only handle so much. We are starting to realize that these are children who are going to be affected at the physiological and safety levels of Maslow's Hierarchy of Needs. It's keeping them from transitioning beyond these levels and they get stuck either at the basic level of physiological or safety. If they're not able to engage in sleep or if they're not engaging in some of their basic self-care like feeding and not getting adequate food, then it's affecting them at the physiological level. If they're feeling unsafe because something in their environment seems like it's some kind of unsafe element, then they're going to be stuck at the safety level.
The other thing we have to think about is consequences of children that have meltdowns, is it shameful? That is going to prevent them from really feeling love and belonging and love and belonging toward themselves which that is another aspect. We always think of love and belonging from other people but it's also part of love and belonging of oneself. That's an important aspect that we have to think about when we're trying to go up this ladder of the Hierarchy of Needs. There are so many hurdles related to moving up this ladder that are really holding children back.
Purposes of Behavior
Behavior can really serve the purpose of communication. That is basic information that many of you probably already know, but some of you might not. It's something that people tend to forget about and a lot of professionals that we work with might not know this or they forget about it or they don't appreciate it. A lot of the parents that we work with do not know this information. It is important that we convey that information to them. Behavior may be misinterpreted as a way of getting revenge. This act of defiance or act of opposition are the terms I hear. We tend to perceive behavior as some kind of attack upon us as the adult instead of interpreting it for the language that it is. The child is seeking attention, escaping a task, a person, or the sensory environment or are communicating some kind of want or need. The fourth category of purposes of behavior is sensory which is really unique in and of itself. I always go back to this basic level of let's go back to what behavior is. It is not revenge on you, it is not some kind of opposition to hurt your feelings and it is not, a complicated thing that we like to think of in our head. It's going back to these three basic levels of communication and let's try to figure out what it is. Let's interpret it just like we would interpret it if it was in a different language. If it was Chinese, we would have to interpret it. It is a different language.
Sensory, Behaviour or Both?
There are three types of behavior. They are whether attention-seeking, a want or a need, or avoidance. Behaviors are dependent on antecedents. That means there is a trigger that is consistent. You can see every single time that a trigger will be there. It is consistent and that will tell you, it is a behavior. So, therefore, it's predictable and it will be responsive to a behavior program. A functional behavior plan will be effective for a behavior situation that is predictable and depends on that trigger. The function, therefore, is the attention-seeking, this communicating a want or a need, or avoidance.
Sensory is not dependent on an antecedent. There is no trigger and it occurs regardless of the circumstances. One of the things that will kind of tell you it is a sensory issue is they'll tell you, "It seems like it happens for no reason." Another red flag for sensory could be no benefit seen when a behaviorist or school set up a positive behavior program or functional behavior program. It could also mean that they didn't figure out what the behavior was correctly, but oftentimes, it means it's sensory and here's where it gets a little confusing. The function is escape or avoidance. Now, that doesn't mean it's the same as the escape or avoidance of the behavior, it means that it's escape or avoidance of a sensory input that is activating the system at a level where the sympathetic system is activated.
Sensory Processing Concepts
Some of you might have heard sensory processing as sensory integration. We are talking about the ability to register and then modulate sensory information, which is really kind of that basic level of processing sensory information. You have to figure out what is it, and then you have to organize it so that you can respond to the situation's demands. It's a very challenging situation for children to do. Our body has to go through this whole process of doing this and so there is an opportunity for things to go awry. The term modulation is simply the ability to notice and regulate the stimuli and respond in an appropriate manner. A lot of children have dysfunction at this level. They tend to either modulate at a level where they don't notice it enough or they notice it too much. It's excessive (hyper) or not enough (hypo). Then we have these neurophysiological processes related to modulation. They are habituation and sensitization. Habituation basically just means that over time, if I am repeatedly experiencing an input, I do not notice the input anymore. So, I want all of you to go ahead take one of your forearms and place it over your other forearm or you can place it over your hand. So, you've got your right hand over your left hand and eventually, you don't really notice it. It kind of becomes one hand. That is habituation. If any you have worked with Kinesio-tape, you know when you first put it on, it's like, "Oh, I notice the Kinesio-tape," and then eventually you don't even notice it anymore, that is habituation. Sensitization is when you're repeatedly exposed to something and it actually becomes more and more bothersome over time. For example, how many of you are bothered by the tags on your shirts? Anybody bothered by headbands or bangs? So, it's really the opposite of desensitization. This can be what happens to some children when that tag is touching them and they notice it more and more to finally, they just can't take it anymore.
Sensory Inputs
The brain processes multiple sensory modality inputs. Most of you are familiar with vision (seeing), auditory (hearing), olfactory (smelling), tactile (touch), vestibular system (movement-related), and taste. Interoception is awareness of your bodily functions and your bodily systems. That would be hunger and a full feeling. It also is your emotions and that feeling of emotion. There is a reason why we call it butterflies in the stomach when we are nervous because there is a feeling involved. That is interoception. Have you ever worked with a child that lacks that awareness of having to go to the bathroom or being hungry? That's because he or she is under modulating interoception. The message is not received and that's a tricky situation because they don't know they're hungry, they don't know they're full, they don't know that they have to go to the restroom and that's one that is often forgotten about. And then, of course, there's also proprioception(the awareness of your body in space), which is a really important piece of the puzzle. Activity level is also included and in your handouts, I added it with a little asterisk next to it. This is because it's included in the sensory profile sometimes from when you've done. The reason why I put it there is because when kids are really busy with things, it sort of creates an experience or a perception of intensity that they will respond to and it's something just to keep in mind.
Sensory Dysregulation
There are several types of models of sensory dysregulation. Winnie Dunn's model has four quadrants. The four quadrants are overly responsive or under-responsive and then an active seeker or one who doesn't seek at all (they're active or passive). The kids that would be in trouble with regard to meltdowns are your sensory sensitive kids who are bothered by input but don't do anything about it and your sensory avoiders who are bothered by input and try to block it out. Lucy Jane Miller's Nosology is more of a diagnostic category of dysfunction. Figure 1 shows her categories and she has the modulation dysfunctions. The over-responsive category is very similar to what Winnie Dunn talks about with being sensory sensitive or sensory avoiders. This would be a child who reacts negatively to sensory input and has meltdowns., They are going to refuse to participate in certain activities and will have aggressive behavior because they will see this as a threat. Under-responsive kids, now if you know Winnie Dunn's terminology, these would be considered your low registration kids and they would be considered sensory seekers sometimes. They would be the active ones sometimes but they're just not aware. They have a limited or decreased response to sensory stimuli. For example, he or she could walk in a room and are not aware of it. These are the kids that have can have a messy face and not realize there is stuff all over their face. They are always a little disheveled. They don't notice injuries. They lack energy and they are not as prone to meltdowns. Sensory seekers on Lucy Jane Miller's nosology are called sensory cravers and they have a significant need for sensory stimuli. For example, they put things in their mouth, they smell things, they touch others, and they tend to have poor safety awareness. They tend to be high energy level. Depending on the true situation, they might be apt to behavioral issues, but not so much a meltdown.
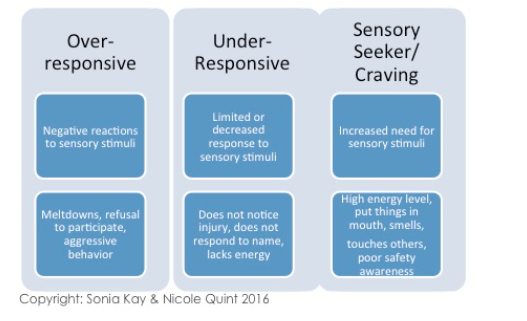
Figure 1. Sensory Dysregulation.
Motor Based Postural Disorders
Postural disorders are significant, especially for many of you who work in pediatric physical therapy. Figure 2, shows is Lucy Jane Miller's Nosology of the motor based postural disorders. There are two of them, postural and dyspraxia.
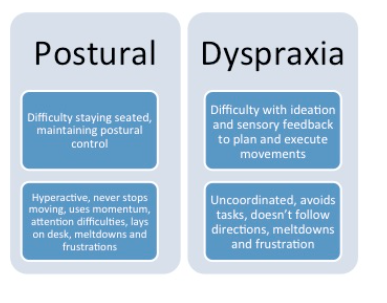
Figure 2. Motor Based Postural Disorders.
Postural control disorder. Postural control disorder has to do with your low tone kids. These children have difficulty staying seated and they have difficulty with postural control. They lack the righting reactions or they are inconsistent with them. They lack their equilibrium reactions. They have difficulty with their ability to maintain supine flexion and prone extension. They tend to be categorized as hyperactive sometimes because they don't stop moving, due to lacking stationary postural control. They oftentimes have attention difficulties and will not stay on task. Therefore, sometimes they will look like ADHD kids. They're going to be prone to meltdowns and they can get very easily frustrated.
Dyspraxia. Children with dyspraxia have difficulty with ideation coupled with proprioception and vestibular processing. They are uncoordinated. They avoid tasks and they don't follow directions. They have poor confidence. Meltdowns and frustration are also seen with this group. They don't always have tone issues, but you might see some tone issues with this group.
Sensory Processing Disorder
Sensory processing disorder can be concomitant with ADHD, gifted, autism, and developmental disabilities. It is very significant in children with down syndrome. We are talking here about the kids who have postural issues related to sensory and the kids who have overly sensitive modulation disorders. Sensory processing disorder is in the DSM with autism now, which is helpful in the schools. That has made a huge difference. However, in 2013, the Owen et al. study from San Francisco State, found abnormal white matter in children with sensory processing disorder. SPD was almost included in the DSM-V, it's very political, and at the last minute, they took it out. What they found is it's primarily in the posterior cerebral tracts and it correlates strongly with atypical unimodal and multisensory integration behavior. The nice thing about the study is it pretty much justifies the diagnosis. They performed functional MRI studies and study is included in your references. The study finally validated what we've been talking about for so long and what we all see in the clinic.
Even though some children may not have a sensory diagnosis, we still need to think about their sensory system, whether the diagnosis is fetal alcohol syndrome, bipolar or schizophrenia. Sensory processing disorder is a white matter disorder, so if you've got a diagnosis that is a white matter disorder, it's probably going to manifest into some sensory issues.
Sensory Input and Threat Analysis
Once I figured the neuroscience behind the issue to explain why sensory and meltdowns go together out, it was like, "Oh my gosh, I've been looking at this the wrong way this whole time". I used to look at meltdowns as behavioral as well. You are all familiar with fight-or-flight. If we all went on a camping trip together and the rangers told us that there were bears in the area, we're gonna be a little bit aware or a little bit more cautious than we are in our everyday life. That's typically how these kids are all the time. They're always kind of on heightened alert. So, if we're camping and we're told there are bears around, we're gonna be on heightened alert, that's not our norm, that's these kids norm. Now what happens, as we go outside and we hear a crunch and we hear a growl, that's a message to us that there's something going on that doesn't seem right, it's a threat. So, what happens is our brain stem would be activated and we've already kind of primed it anyway 'cause we were told information that said, "Warning." Then we heard something that validated that warning and so once that happens, that norepinephrine is really saying, "Hey, let's get this system aroused "so that we know that we're ready to go." Then the amygdala gets involved and as soon as the amygdala gets involved and the limbic system gets activated, you're kind of already running in an emotional sense. Dopamine will be released and now what happens is sensory input is going to be received into the body. So if we hear that crunch, we hear some sounds, we see something, whatever it is, it's going to go into two places, the cortex, and the amygdala. The cortex starts to perceive the sensation and it initiates some kind of action as a response. The amygdala now stores the memory and this is very important because once the memory is stored, it attaches a meaning to it. Once that meaning is stored, it's in there forever. The meaning is very important because we can make that meaning become more heightened each time and it becomes sensitive to fight-or-flight. So, really at the end of the day, what happens is once that amygdala is triggered and that memory is triggered and we say, "Oh, that's the bear," you know, we're now going to go into fight-or-flight because we've now figured out it is a threat.
The whole thing really involves a process of moving all this information through the brain from memory to saying, "Uh-oh, "that is the memory, we need to go." What happens is there's a threat versus excitement analysis that happens. I have to figure out, is it a threat or just something exciting and so if it's a threat, then you're going to kick in that whole sympathetic to autonomic process and you're going to go into fight-or-flight. A meltdown is basically going into fight-or-flight.
