Editor’s note: This text-based course is a transcript of the webinar, Manual Wheelchair Mobility: Self-propulsion, presented by Michelle Lange, OTR, ABDA, ATP/SMS.
Learning Outcomes
- After this course, participants will be able to:
- list 3 categories of manual wheelchairs.
- identify optimal manual wheelchair configuration for self-propulsion.
- identify optimal self-propulsion stroke to increase efficiency and decrease injury risk.
Introduction
We will be discussing manual wheelchair mobility today, particularly wheelchairs designed for people to self-propel rather than someone else pushing them.
What We Are Covering In This Series
- Mobility Series
- Augmented Mobility
- Dependent Mobility
- Manual Mobility
- Power Mobility
We are covering several courses in a series about mobility. We started with augmented mobility, then discussed dependent mobility, and in this course, we cover manual mobility, designed explicitly for self-propulsion. Finally, we have a fourth course in this series on power mobility. I would encourage you to check out all of these courses.
What We Are Covering Today:
- Definitions
- Who uses these?
- Assessment
- Components
- MWC categories
- Clinical indicators
- Propulsion
What are these manual wheelchairs? What are the different categories of manual wheelchairs that fit within the self-propulsion category of manual wheelchairs? Who uses this type of equipment? What do we need to keep in mind in terms of our assessment? What are the components of these chairs? What are the clinical indicators for each of these categories? And then finally, we will discuss some specifics about propulsion.
Manual Wheelchair Definition
- A manual wheelchair is designed to provide dependent or independent mobility to a client, as well as support an appropriate seating system.
This might be pretty self-evident, but sometimes in my letters of medical necessity, I need to explain this definition to a funding source. "Without some type of mobility base, we do not have anywhere to put the seating system." With a mobility base, we are supporting the recommended seating system for the client and providing either a dependent or independent form of mobility.
Why Does Someone Need These Devices?
1. Manual wheelchairs may be used for clients who:
- Have no other means of mobility
- Dependent
- Independent
Why does someone need a manual wheelchair? Manual wheelchairs may be used by clients who have no other mobility means, either dependent or independent. Without the manual wheelchair, there is no other way this person can get from point a to point b, from the car into the doctor's office, move around the community, et cetera.
2. Manual wheelchairs may be used for clients who:
- Can ambulate, with or without the assistance of walking aids, but:
- Only for short distances
- With excessive effort
- With fatigue
- Are at risk of falling
Manual wheelchairs can be used by people who have some ambulation, with or without the assistance of walking aids, such as a cane, crutches, a walker, or a gait trainer. The person may ambulate with or without these assisted devices, but only for short distances, with excessive effort, fatigue, or high fall risk. A common myth is, "If my client can walk at all, with or without these aids, we can not recommend a manual chair." However, many people use a manual chair for certain times of the day, for longer distances, for particular environments, or safety.
3. Manual wheelchairs may be used for clients who:
- Use a power wheelchair, but require a back-up in case:
- The power wheelchair is not functioning
- An accessible vehicle is not available
- The destination is not accessible
Manual wheelchairs can also be used for clients who use a power wheelchair but need a back-up. This scenario is a little difficult for funding. Some funding sources will not fund a back-up manual chair, but many will. And, there are times when the power chair may not be working. I wish that were not the case, but wheelchairs break down, batteries run out, et cetera. Until this is addressed, the client cannot use that base, and they need a back-up. It might be that an accessible vehicle is not available. The family's accessible vehicle is in the shop, or they do not have access to an adapted accessible vehicle service that particular day. It could be that a destination is not accessible. Many destinations are not accessible by a power chair. For these destinations, a back-up manual wheelchair is required.
These are the main reasons that someone would require a manual chair. They have no mobility or limited mobility, need a manual chair in certain circumstances, or if they use power mobility, they may require a back-up.
Goals of Use Include:
- Safe and efficient mobility within the client’s environments
- Dependent
- Independent
What are the goals of a manual chair? We want to provide safe and efficient mobility within the client's environment. This might be indoors, outdoors, or out in the community. Medicare stated that if somebody has a wheelchair base, they must require it within their home. That does not mean that it cannot be used outside the house, but they want to ensure this person needs it in their home and that their home is accessible. We want to provide that safe and efficient mobility in these environments, whether or not the client's mobility is independent or dependent.
Who Uses A Manual Wheelchair?
- Clients with:
- CVA
- SCI
- Cerebral palsy
- TBI
- MS
- Muscle diseases
- Other
Clients with CVA, spinal cord injury, cerebral palsy, traumatic brain injury, multiple sclerosis, muscle diseases, etc., may need a manual wheelchair. Sometimes people may require a manual wheelchair for a very short time, perhaps after a hip replacement.
Assessment
- Assessment is typically done with a wheelchair supplier
- Lightweight, Ultra-Lightweight, Pediatric, and Bariatric manual wheelchairs are Complex Rehab equipment
- Complex Rehab is typically recommended by a professional who is certified:
- ATP: Assistive Technology Professional
- SMS: Seating and Mobility Specialist
- These are obtained through RESNA
- Rehabilitation Engineering and Assistive Technology Society of North America
Assessment is typically done with a wheelchair supplier and a clinician. The clinician looks at the clinical and functional aspects of the wheelchair, but the wheelchair supplier knows the equipment well and can match specific client parameters to product features.
Lightweight, ultra-lightweight, pediatric, and bariatric manual chairs are considered complex rehab equipment. Complex rehab equipment is typically recommended by someone with a specific credential, ATP, or Assistive Technology Professional. This is a certification from RESNA, the Rehabilitation Engineering and Assistive Technology Society of North America. Depending on the funding source, a person must have an ATP certification to recommend complex rehab-level chairs.
Some suppliers and clinicians may also have an additional certification called the SMS, Seating, and Mobility Specialist. The ATP is a more general assistive technology examination, whereas the Seating and Mobility Specialist certification is an extra layer of expertise in this area. When we are assessing, the supplier must have adequate experience, including an ATP certification.
- Considerations include:
- Strength, range of motion, muscle tone, and orthopedic status
- Cardiopulmonary status and fatigue
- Potential for change in function or size
- Positioning needs
- Environmental needs
We need to look at the client's strength, range of motion, muscle tone, and orthopedic status during the assessment. These areas are going to dictate their seating system needs and their ability to self-propel. This does not mean that you need to spend hours on standardized testing. You need to look at the client's strength and range of motion that are required to self-propel a manual wheelchair. The client's muscle tone and orthopedic status are also going to impact seating.
Cardiopulmonary status is another area to assess as this person might experience difficulty during self-propulsion if their heart rate goes up or their fatigue is excessive. There are some clients out there who absolutely could self-propel a manual chair. However, due to the cardiopulmonary cost, they need power mobility.
We also need to keep in mind the potential for change in functional abilities or size. If the client has a progressive condition, we need to decide if a self-propelling manual chair is appropriate. It might suit their needs now, but it may not after some years. Size changes are certainly expected in the pediatric population, but adults change in size as well.
Positioning in the manual wheelchair is incredibly important. If someone is not positioned well, they will not be able to propel the manual wheelchair very well.
Finally, we need to look at the environment. What type of environment is this person in most of the day? Do they live on smooth linoleum or shag carpets? What are their community needs?
Components
- Each wheelchair contains various components
- These vary with wheelchair category
- These affect the performance of the wheelchair
What are the components of these manual wheelchairs? Each wheelchair contains a variety of features. Figure 1 shows some of the details on a lower-end manual wheelchair.

Figure 1. The components of a manual wheelchair. Click to enlarge the image.
These components will vary with the wheelchair category and affect the performance of the wheelchair. It is crucial to be familiar with some of the terminology so that we know what everyone is referring to when we are working with a team. There is the rear wheel that is comprised of the tire, the push rim, and spokes. Sometimes, there is a mag wheel instead of spokes where larger plastic sections connect the axle to the tire. There are also "brakes," but the correct terminology is wheel locks. They lock the wheel in position to keep the chair from rolling, especially on an incline.
There are footrest hangers and footplates that are part of the footrest assembly. The front wheels are referred to as casters. There are various style armrests that we can get for the client. The push handle on the back allows caregivers to push or assist the client.
For the seating, there is a backrest and seat. This particular chair has simple upholstery, but this is usually inadequate for our clients. Typically, we put some type of other seat and back on here. The upright bars that hold the back are called back canes, and the seat rail is where the cushion is attached.
Manual Wheelchair Categories
- Standard Wheelchair (K0001)
- Standard Hemi Wheelchair (K0002)
- Lightweight Wheelchair (K0003)
- Lightweight Wheelchair (K0004)
- Custom Lightweight and Ultra Lightweight Wheelchair (K0005)
- Pediatric
- Bariatric
- Specialty
These manual wheelchair categories are dictated by funding. These billing codes are from Medicare, and many other funding sources follow these guidelines. In addition to these codes, we also have chairs explicitly designed for the pediatric population, the bariatric population, and a few specialty chairs in addition to these codes. They are typically not covered by funding sources, but a client might pay for these out-of-pocket.
Standard Wheelchair- K0001
- Medicare K0001
- Dependent wheelchair
- Weight over 35 pounds
- Limited sizes, adjustments, modifications, seating
Standard wheelchairs are called a K0001, and an example can be seen in Figure 2.

Figure 2. Example of a standard K0001 wheelchair.
This K0001 standard wheelchair is what we saw in the picture with the labeled components. Again, Medicare calls this a K0001 or "K1." These weigh over 35 pounds and are hard to propel. There are limited sizes and adjustments on these. By size, I mean seat depth, seat width, and back height choices. This model comes in generic sizes that may not match up the size requirements of your client. There is also not a lot of adjustment within the frame, and it does not support many seating options.
- Appropriate client:
- A client who needs a temporary wheelchair and is dependent for mobility
- Even if a client could propel this, other categories are recommended for self-propulsion
Who is appropriate for a standard wheelchair? I am hard-pressed to say anyone is suitable for this frame. It might work for someone who needs a temporary wheelchair and is dependent for their mobility. Even if a client can manage to propel this, other categories are recommended for self-propulsion because this is just too heavy.
Standard Hemi Wheelchair- K0002
- Medicare K0002
- Standard manual wheelchair with a lower seat to floor height to allow for foot propulsion
We then move on to the Medicare K2, the standard hemi wheelchair (Figure 3).

Figure 3. Example of a standard hemi K0002 wheelchair.
The "K2" is a standard manual wheelchair that has a lower seat to floor height. This is specifically designed for foot propulsion. "Hemi" refers to people who have had a stroke, with one side of the body being more involved than the other. This manual wheelchair is challenging to self-propel with both hands, or the person with hemiparesis may propel in circles. There are some one-handed options that we will talk about in a little bit, but most clients move these with one hand and one foot, so they need a lower height.
One challenge is that if someone else is pushing, the client needs to hold their feet against gravity because there may not be footplates. If we put footrest hangers on this wheelchair, since it is a lower design, the footrests pull the legs up so that they are not on the cushion surface, which puts a lot more weight on the pelvis area. This could lead to pressure concerns.
- Appropriate client:
- Hemi refers to decreased control on one side of the body, such as clients who have had a stroke. This client may propel with one arm and one foot
- This is not an ideal wheelchair for any form of self-propulsion
These are often used by people with self-propulsion by one foot and one hand, but this is not an ideal chair for any form of self-propulsion. Again, it is too heavy and does not have a lot of adjustments to allow us to optimize that propulsion or seated position.
Lightweight Wheelchair- K0003
- Medicare K0003
- Less than 36 pounds, 28 pounds average
- More sizes available, but little or no frame adjustments
- Limited options and accessories
We then move on to a lightweight wheelchair, a "K3" shown in Figure 4.

Figure 4. Example of a lightweight K0003 wheelchair.
These weigh less than 36 pounds at an average of 28 pounds. More sizes are available for seat width, seat depth, and back height, but there are little or no frame adjustments, options, or accessories on these lightweight wheelchairs. Frame adjustments are critical for providing seated angles like the seat to back angle to best support someone's postural needs and optimize self-propulsion.
- Appropriate client:
- A client who cannot propel a Standard wheelchair but can propel a Lightweight wheelchair
- Not designed for long term use or extensive self-propelling
You could use this for clients who cannot propel a standard wheelchair but can propel this lightweight one. However, it is not designed for long-term use or extensive self-propelling. This frame might work well for someone who only sits for short periods, like from the car to the doctor's office, or temporarily uses it. If someone is going to be self-propelling many hours a day or over, say the next five years, we need to look at something else.
Lightweight Wheelchair- K0004
- Medicare K0004
- Weigh less than 34 pounds, average 26 pounds
- More sizes, options, and accessories
- Minimal frame adjustments
- Minimal adjustable axle plate
We then move to the K4s.

Figure 5. Example of a lightweight K0004 wheelchair.
The K4 is also considered a lightweight wheelchair, like the K3, but these average 26 pounds. It is only a difference of about two pounds from the K0003, but this can make a big difference for someone self-propelling. There are also more sizes, options, and accessories than the K3s. However, it still has some frame and adjustable axle plate adjustments essential for correct seated angles for clients. The wheels are stationary and cannot be moved on the K1, K2, and K3 wheelchair models. This standard wheel position is the best place for stability but not for self-propulsion.
When we get to the K4, we now have an adjustable axle plate that allows us to move the rear wheel forward to optimize self-propulsion. There is not a lot of adjustment on this axle plate, but it can be moved vertically so that the center of the axle is in a better place in relation to the client's hand.
We will talk more about propulsion later, but the K0004 is a little lighter weight, has more frame adjustment, and has some adjustment in the axle.
- Appropriate client:
- A client who cannot propel a lesser category of wheelchair due to weight and set-up
- Frame adjustments optimize self-propulsion
This is appropriate for a client who cannot propel a lesser category of wheelchair due to the weight. Configuration options and frame adjustments can optimize self-propulsion, but not as much as our most adjustable chairs that we will talk about here in a second.
In our documentation, when we are recommending a manual chair, we must explain why the less costly category is not appropriate. For example, if we recommend a K4, we need to explain why a K3 will not meet a client's needs in our documentation. The supplier can be beneficial in this process. They are familiar with the wording a particular funding source needs. Ethically, they should not write that out for you, but they can give you some guidance regarding some of the justification you can use to explain why a particular category is required.
Custom Lightweight & Ultra Lightweight- K0005
- Medicare K0005
- Weigh less than 30 pounds, as low as 17 to 18 pounds
- The greatest degree of options:
- Size
- Frame adjustments
- Suspension
- Casters
- Designed to maximize self-propulsion efficiency and reduce RSI risk
We finally move into our K5 chairs that are custom lightweight and ultra lightweight, as shown in Figure 6.

Figure 6. Examples of rigid versus folding K0005 frames.
I wish we could recommend this category for everyone as I feel they are the best wheelchair option. I do not mean best in terms of being cool-looking or having cool colors, but these have a lot of features that optimize self-propulsion and protect our clients from injury, particularly over the long term. As before, we need to justify why a lesser category will not meet the client's needs. Some weigh less than 30 pounds, and some are as low as 17 to 18 pounds. It is pretty amazing how lightweight they are.
You might be thinking, "My client weighs 200 pounds, so what difference does it make to go between 17 pounds and 30 pounds?" Think of it this way. If you have ever ridden a very lightweight bike before, there is quite a difference. For example, I happen to have a $69 Huffy that is a beast. When I have had a chance to hop on someone's lighter bike, I have felt like I could ride for miles and miles. The weight makes a huge difference. If you have a chance, I would encourage you to try a standard wheelchair, like a K1, and push it around. Then, hop in one of the ultra lightweights. There is a world of difference in function between one category and another.
The K0005 category has the most significant degree of options. And, in terms of size, they can get precise. Suppose a client has an unusual combination of seat width and seat depth. In that case, they can be fitted typically with this style as there is a lot of adjustment on the frame and a wide variety of size options to accommodate any seating system on the market. It can also meet the client's specific seating angle requirements, particularly seat to back angle, the angle at the knee, and the footrest angle. There is even some suspension available. Suspension is not used only for comfort. As someone is self-propelling over a surface, there can be a great deal of vibration that comes up through the frame, leading to fatigue and eliciting increased muscle tone or spasms. Suspension dampens vibration and the bumps and jolts of the road.
Casters are the little wheels in the front, and this category of wheelchair has many caster options. If we choose a very small caster, it allows someone to turn more readily, but a larger one makes it easier to manage varied terrain. We will talk a little more about casters in a few minutes.
The main goal of this category of manual wheelchairs is to maximize self-propulsion efficiency and to reduce the risk of repetitive stress injuries. We know that people who have used a manual chair for many years develop significant repetitive stress injuries in the shoulder, the elbow, the wrist, and the hand. If we can recommend an optimal frame, we are helping out clients avoid some of these problems.
- Appropriate Client:
- Any client who is self-propelling using both arms for a significant time period
Who are an appropriate candidate for these custom lightweight and ultra lightweight chairs? Any client who self-propels using both arms for a significant time period needs to be using this category of chairs. It is essential, and this is what we need to include in our documentation.
- Folding and Rigid frame options
- Folding is easy to transport and often has more growth or other frame options
- Rigid frames are lighter, more durable, and more energy-efficient
These ultra lightweight chairs come in folding and rigid frames. Those that fold in a side-to-side configuration can sometimes be easier to transfer or transport. Rigid frames can also be easily transported by removing the rear wheels or folding the back down to create a small box (Figure 7).

Figure 7. Example of a rigid manual wheelchair.
Wheelchairs with folding frames also allow more growth options because the X frame underneath the seat can be replaced to widen the frame. Rigid frames are usually lighter than folding chairs because they do not require a folding mechanism. Rigid frames also tend to be more durable because there are no potential breakage points like a folding frame, and they are more energy-efficient as the client's energy goes into propulsion. In contrast, a folding frame takes some of that energy via the moveable parts. There are newer hybrid frames that lock so that less energy is wasted.
- Durability
- Research has demonstrated that over the lifetime of the frame, ultra lightweight wheelchairs are more cost-efficient than other less costly frames.
- Fitzgerald, Shirley G., et al. "Comparison of fatigue life for 3 types of manual wheelchairs." Archives of physical medicine and rehabilitation 82.10 (2001): 1484-1488.
Durability is essential, and there has been a lot of research that has compared the durability of various categories of chairs. RESNA (Rehabilitation Engineering and Assistive Technology Society of North America) also has standards for manual wheelchairs. They should sustain a certain amount of drop forces going over a curb or a certain amount of rotation in the rear wheels before anything breaks. Using testing facilities, they have found that ultra lightweight chairs are more cost-efficient than other less costly frames because they last longer. This is important to know because funding sources will say that ultra lightweight chairs cost more. It should cost a lot more than a K1 because it is a much more efficient, sophisticated base. The good news is that it is far more durable and should last the client a much longer time, making it a more cost-efficient choice than even those standard wheelchairs.
Pediatric Manual Wheelchairs
- Accommodates smaller dimensions
- Growth varies from frame to frame
- Low seat to floor height
We then have pediatric manual chairs that are designed to accommodate smaller dimensions (Figure 8).

Figure 8. Example of a pediatric frame.
Growth is a significant factor in pediatric chairs. These wheelchair frames have a tremendous amount of growth, but they will vary from frame to frame. Some of these start with a very low seat to floor height (as in Figure 8) to allow the child to complete stand pivot transfers. They also need to have something they can sit on rather than have to climb up.
Bariatric Manual Wheelchairs
- Bariatric manual wheelchairs offer wider frames and higher weight limits
- Heavier and wider frames are harder to push
- Wheels are too far away from the client
- May not fit through doorways
Bariatric manual chairs offer a wider frame width and have higher weight limits (Figure 9).

Figure 9. Example of a bariatric frame.
Each manual chair on the market has a recommended weight limit, and this is the highest someone should weigh to use the wheelchair safely. If I see a client within 5-10 pounds of that weight limit, I will be pretty concerned that they could exceed that weight limit. I would most likely move them into a bariatric chair.
There are different categories of these bariatric chairs because there are people who are just over the weight limit and some who are at a much higher weight and require a more specialized frame that can accommodate that. A frame that weighs more and is wider is harder to push. Figure 9 is an example of a very wide frame. A caregiver would be quite challenged to reach both of those push canes and push the chair efficiently. Also, the wheels are far apart, thus making it more difficult to self-propel. And, if we recommend something wide enough for the client, it may not fit through the doorways.
Bariatric seating can be a challenging area of wheelchair seating and mobility. We might opt to place someone within a seating system that is a little narrower than we usually would recommend. While it is important to accommodate excessive tissue laterally, the goal is to ensure this client can still get through doorways or a widened doorway.
Specialty Wheelchairs
- Sports
- Generally, these are a second wheelchair, often out-of-pocket payment
Specialty chairs can be used for sports and recreation. Generally, this type of wheelchair is an optional one, and the family buys this out-of-pocket. In Figure 10, the left wheelchair is designed for basketball and the right for recreational use.

Figure 10. Examples of specialty wheelchairs.
- All-terrain
There are also all-terrain manual wheelchairs available.

Figure 11. Example of an all-terrain manual wheelchair.
Figure 11 shows one with good suspension and outdoor specialty tires. These could be used on a dirt trail as an example. However, the client will need good strength to use this. It is often used as a secondary chair as well. Some clients have more than one set of tires and will change them out depending on the activity. Figure 11 has heavy-duty tires. Figure 12 shows a beach wheelchair.

Figure 12. Example of a beach wheelchair with wide tires.
There are a number of these available to purchase, and there are also places that will rent them or provide them for free on certain beaches and even national parks. Here in Colorado, we have the Great Sand Dunes, National Park. You can check out a wheelchair like this so that someone can be propelled over the sand dunes. This is not designed for self-propulsion.
I am amazed how often someone will recommend a manual chair without really being familiar with all the various product options. I overheard a doctor telling a family to go to the local drug store and purchase a wheelchair out-of-pocket. Transport chairs are something we covered in the dependent mobility course. While they are inexpensive, they rarely meet someone's needs and are only designed for quick use for transportation.
Self-propulsion Considerations
- Weight
- Rear-wheel placement
- Optimize efficiency
- Stability vs. maneuverability and turning radius
- Self-propulsion pattern
- Camber
- Front caster
- Size
- Loading
Now, we are going to talk about specific considerations for self-propellers. These include the weight of the frame, the placement of the rear wheel, the pattern someone is using with their arms for self-propulsion, the camber of the wheel, and some aspects of the front caster.
Weight
- Generally, the lighter the wheelchair, the more efficient it is to propel
- This includes the weight of components and seating
We have talked quite a bit about weight being a specific characteristic between these various manual wheelchair categories. Generally, the lighter weight the chair is, the more efficient it is to propel. This overall weight includes the weight of the components and the seating system. When looking at the weight of a wheelchair, not all wheelchair manufacturers report the weight the same way. Some manufacturers may include only the frame's weight without the footrest hangers, without the seating, and without even the rear wheels. We need to know what components the manufacturer includes in their wheelchair weights to compare apples to apples. Sometimes if you look carefully on the website, you can see what that chair weighs with footrest hangers and rear wheels. Then, you have to keep in mind the weight of the seating system. For instance, you do not want to put a super heavy seating system on top of an ultra lightweight wheelchair because this negates a lot of the benefit of that lightweight chair. Instead, we need to choose seating components that still meet the client's postural needs but weigh as little as possible. In a dependent chair or a power wheelchair, the seating system weight is not as critical.
Rear Wheel Placement
- If the rear wheel is placed behind the client, the wheelchair is more stable, but the propulsion stroke is less efficient
- If the rear wheel is placed too far forward, the wheelchair will be tippy rearward.
- Balance of stability and maneuverability
- Placement for the ability to do “wheelies”
The next consideration is rear-wheel placement, specifically for self-propulsion. If the rear wheel is placed behind the client (where it is placed on most lesser categories of manual chairs), the wheelchair is more stable. However, it is hard to tip the wheelchair if the wheel is too far back, but the client has to reach further behind them for propulsion. This is not good for the shoulder, and it is not a biomechanically efficient position, as if the wheel is directly below the client's shoulder. If the rear wheel is placed too far forward, the wheelchair tends to be tippy. We have to find a balance between stability and maneuverability. Additionally, many people who self-propel will use wheelies, not just to show off, but to functionally get down a steep ramp like this gentleman's doing in Figure 13 or to get up and over a curb. We also need to make sure the placement of the rear wheel is optimal to allow a person to safely do a wheelie without tipping over.

Figure 13. A gentleman doing a wheelie to descend a steep ramp.
There are some excellent training programs out there for people who use manual wheelchairs. One is the wheelchair skills test and training program by Lee Kirby. There are many resources, some for free and some for a cost, that can help you train someone to use their manual wheelchair. There is also a book called "The Manual Wheelchair Training Guide" by Peter Axelson and other co-authors.
In terms of wheel placement, you want the client's shoulder and the tip of their middle finger to align with the axle when fully extended. Figure 14 shows an example of this.
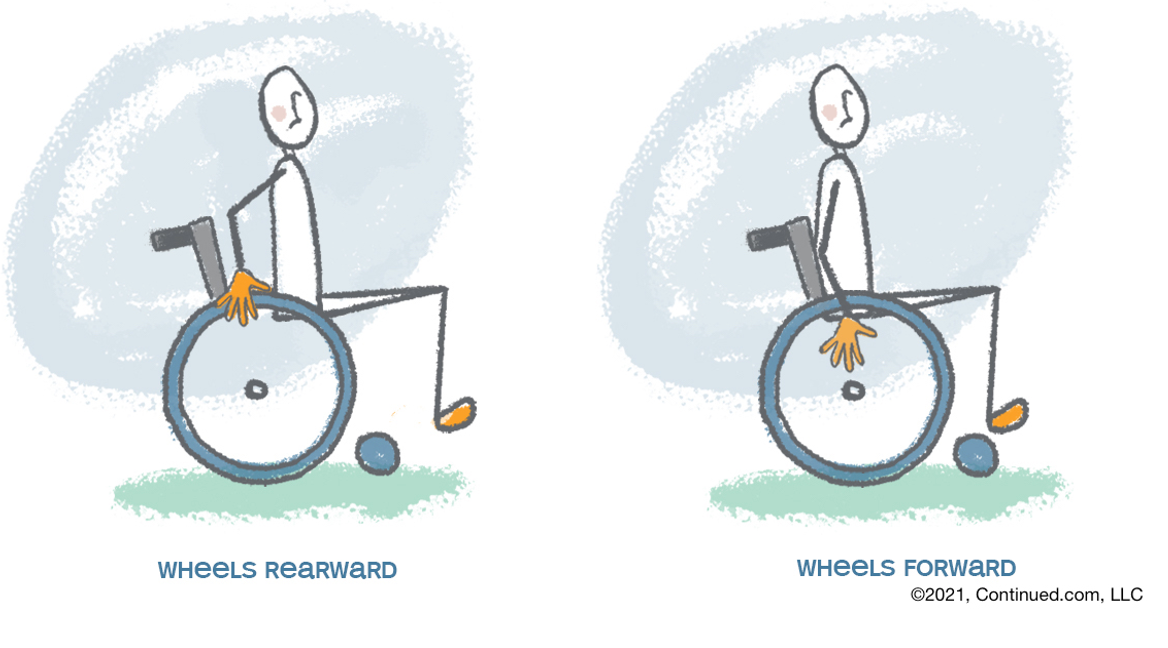
Figure 14. Correct wheel placement for more efficient wheelchair propulsion.
A lot of research supports wheelchair wheel placement, especially by the Paralyzed Veterans Administration (PVA). In the left image, you can see that the wheel is too far back for the person, and their hand will be in front of the center of the axle. And again, ideally, we want that axle in line with the shoulder and with the tip of the middle finger right at the center of the axle.
Self-Propulsion Pattern
- Single loop most efficient
- Reduces RSI risk
- Long stroke
- Minimal impact upon grip
- https://www.rehab.research.va.gov/JOUR/05/42/3suppl1/pdf/boninger.pdf
What is the best propulsion pattern? There are different patterns that people tend to use, but a single loop is the most efficient. We will see a video of this in a moment. There is also an excellent research study that goes through these different patterns listed above. We want the client to use as long of a stroke as possible. They need to reach far back behind them, grab that wheel, and then push forward. We also want minimal impact upon their grip. So when their hand first hits the wheel, we do not want that to occur with a great deal of force to cause jarring through the hand, wrist, elbow, and shoulder. The less force, the better because the client may be doing these hundreds, if not thousands, of times a day over many years. It is vital to train clients in the single loop as it reduces the repetitive stress injury risk. We want them to use a long stroke without much impact upon contact with the hand on the wheel.
We are going to watch a 4-minute video that highlights this pattern. This video goes through some considerations of wheelchair configuration to optimize someone's self-propulsion to minimize injury risk. This is from the University of Washington, and we thank them very much for allowing us to use this. This video is from a specific wheelchair skills video series. They have some other videos, and these are all available on YouTube.
SCI Empowerment Project: Video 13 Wheelchair Pushing- Design

Video 13, wheelchair pushing, wheelchair design. Good form when pushing a wheelchair can help you avoid arm pain and fatigue over years of use. But form involves more than technique. Propelling well depends on having a custom wheelchair fit that encourages upright posture as well as wheels that are easy to reach and push. Your posture affects your propulsion form, and your wheelchair influences your posture. Sitting with a slouch causes neck and arm pain when wheeling because the joints are in a harmful position. Sitting upright will protect your joints and muscles but may feel stable. If you do feel unstable, have too much pain, instability, or tightness to have good posture, you may need adjustments to your wheelchair cushion, backrest, or frame to support you in a comfortable upright position. If you sit too high above your wheels, you'll not be able to reach the hand rims effectively. A guideline is that you should be able to touch the center of the wheel with at least the tip of your middle finger or even your palms when you dangle your arms at your sides. Secondly, you will not be able to reach the hand rims well if you're sitting too far in front of the wheels. This is because you will have to extend your arms too far back to reach your wheels, which will strain your shoulders. Instead, the wheels should be as far forward as possible without making the wheelchair too unstable. An unstable wheelchair tips back into a wheelie too easily, which can make pushing your wheelchair, stressful, tiring, and potentially dangerous. Wheels that are too far out to the sides are hard to reach. You may need to order a narrower wheelchair and cushion the next time you get a wheelchair to bring the wheels closer to your body. Even when you have good posture with well-positioned wheels, you will still have pain and fatigue with pushing the wheelchair if the tires start to go flat. Keep a pump and spare inner tubes with you at all times. Get into the habit of checking the tire air pressure every couple of weeks. If you tend to push on hard, smooth surfaces, like tile floors, most of the time, you'll have an easier time pushing a high-pressure, low tread tire.
In contrast, if you typically push your wheelchair over gravel and grass, you may want a pair of tires that are low pressure with thick tread. However, low-pressure thick tread tires are typically too hard to push for everyday use on indoor surfaces or sidewalks and should be reserved for specific activities. You may find that your hands slip on the smooth hand rims, especially when the rooms are wet or if your hands are numb or weak. Your hands may ache or tingle when you grip the small tubing of standard hand rims. Consider alternatives such as rims with coatings and rims with wider oval tubing. If you struggle to maintain a good wheelchair pushing form, you may need to think about other wheelchair products on the market. You may want to explore a mechanical or motorized attachment for your ultralight wheelchair or potentially a power chair. A wheelchair seating clinic can help you make these decisions over your lifetime. Continually re-evaluating your wheelchair seating and technique will help you preserve your shoulders, avoid pain and weakness, and be as independent as possible as time goes on.
Thanks to the University of Washington for a great series of videos.
Camber
- Camber increases stability and maneuverability in turning
- Camber increases the overall width
Camber increases the chair's stability and maneuverability during turning, but it also increases the chair's width (see Figure 15).

Figure 15. Examples of wheel camber.
If we look here on the right, this is a chair used for sports like tennis. Part of the reason for this huge camber is as the person reaches over to hit the ball, the chair stays stable. The person can also turn on a dime as it is very maneuverable. However, it is not so great for getting through your bathroom doorway. We can sometimes add just a little bit of camber to make it easier to turn and increase stability for the typical client and keep the chair narrow for doorways.
Casters
- Front caster
- Size
- Smaller allows tight turns, less interference with footplates
- Larger is better for varied terrains
- Loading
- It is important to not position the client in the wheelchair so that the front casters are “loaded.”
- Impedes turning
- Increases wear
- Size
Casters come in many styles, including rollerblade-style ones that light up when you push them. Examples are seen in Figure 16.

Figure 16. Types of casters.
Smaller casters allow for tight turns with less interference with the footplates, which sit above the smaller ones. However, small casters tend to get caught on cracks in the sidewalk and thresholds. Larger size casters work better for varied terrain. Front casters cannot be easily swapped out like rear wheels. A caster that is in between a small and large does pretty well in a variety of environments.
You may have heard of something called front caster loading. If the person is seated well forward on the chair, they have a lot of their weight over the front casters, making it difficult to turn. It also increases the wear of the casters. This is an important consideration, and the supplier should have some options.
Alternative Propulsion Patterns
- The most efficient means of self-propulsion is 2 hands
- If the client is unable to do so, a power wheelchair may be indicated
- If the client only needs to move short distances, time is not an issue and surfaces are level and flat:
- One hand
- One hand, one foot
- Both Feet
The most efficient means of self-propulsion is using two hands. If the client is unable to propel with both hands, a power chair may be indicated. If the client only needs to move short distances, time is not an issue, and all of their surfaces are level and flat, we can look at alternative propulsion patterns like one hand, one hand, one foot, or both feet. Even though it's possible to propel this way, we do not want to do so for long distances or long periods as they are very inefficient.
One Handed Propulsion
- A special wheelchair modification is required
- Dual Rims
- Requires larger hand and very good grip strength
- Levers
- Not available in the US at this time
- Dual Rims
For someone who is using only one hand to propel, there are some special wheelchair modifications available. One is a lever style, but it is not available in the US at this time. It has been in the past and probably will be in the future.

Figure 17. Example of lever-style rims on a wheelchair.
You push back and forth on this lever to move the chair forward. The one pictured here has two levers, but there is also a one-level style for using one hand. There are also dual rims, as seen in Figure 18.

Figure 18. Example of dual rims on a manual wheelchair right wheel.
If the person pushes both rims at the same time, they will go forward. If they grasp just the inside rim, they will move to their left side, and if they grasp the outside rim, they will go to the right. It requires a larger hand to span these rims and good grip strength to push them both forward.
One Hand One Foot
- Used for short distances, often by clients who have had a stroke
- Seat to floor height must be low
- Slow, takes a lot of energy
- May pull the pelvis forward
Some clients do use one hand and one foot often after a stroke, and this is propelling method is used for only short distances. The seat-to-floor height has to be low to allow for this propulsion method. It is slow and takes a lot of energy. Whenever a client uses a foot to pull the chair forward, the pelvis also tends to pull forward.
Both Feet
- Requires low chair
- Generally, it pulls the pelvis forward into a posterior pelvic tilt
The same issues are seen in those that use both feet.

Figure 19. Example of a client propelling a wheelchair with both feet.
The pelvis is pulled forward as the client pulls their feet along the floor.
Dilemmas
As we wrap up, I want to talk about a few dilemmas that we have to deal with.
Long-Term
- Many Long-Term Care facilities will only use manual wheelchairs that are already in their “fleet.”
- These are typically inadequate in terms of seating and mobility
- Options?
- Advocacy
- Education
Many long-term care settings will only use manual wheelchairs already in a storage room or their fleet. These bases tend to be somewhat inadequate in terms of seating and self-propulsion. What can we do? It is essential to educate the people who are making purchasing decisions and explain the difference in functionality and durability in these bases and the cost. It is also important to advocate for a wider variety of wheelchair options as a part of that fleet to meet clients' needs.
Medicare
- Medicare and other funding sources often change their regulations
- Funding may be limited
- Work with the supplier to learn the latest requirements and ensure that your documentation is adequate for funding approval of appropriate equipment.
- Denials do not always mean no!
- Provide further education
- Advocacy
Another dilemma is that Medicare and other funding sources often change their regulations. As such, it is hard to keep track of what the current funding limitations are. Thus, it is essential to work closely with the suppliers to learn the latest requirements to ensure adequate documentation and funding for your recommendations. Remember, it is not uncommon to get a denial. It can be very frustrating, but denial does not mean no.
There are a couple of options for denials. Depending on the funding source, there is usually an appeal process that the family could follow. They are not suing anyone, but instead, they are taking advantage of their rights within the funding sources' requirements. I often write additional documentation when a funding source has further questions or is denied something, and most of the time, we can overturn that denial. It is important to get in there and not give up. If we all roll over and say, "Oh well, it's denied," unfortunately, we are going to see a lot more denials.
Alternative Drive Mechanisms
- Providing assist for self-propulsion of a manual wheelchair
- Lever drives
- Arm-crank drives
- Geared hubs
- Reverse push rim drives
- Pushrim-activated power assist drives
Some alternative drive mechanisms are available as well. These assist self-propulsion on a manual chair. They include lever drives, arm crank drives, geared hubs, reverse push rim drives, where you pull instead of push and push rim-activated power-assist.
Mobility Hierarchy
- Dependent Manual Wheelchairs
- Independent Manual Wheelchairs
- Designed for self-propulsion
- Alternate Drive Mechanisms
- Power Wheelchairs
It is essential to keep in mind our hierarchy for wheelchair recommendations. We may recommend an alternative drive mechanism, a hybrid, between independent, self-propulsion, and a power chair.
Goal
- Improved mechanical efficiency
- Maintain transportability, versatility, and aesthetics of a manual wheelchair
DiGiovine & Berner, 2018
The goal of these is to provide improved mechanical efficiency to the client but maintain the transportability, versatility, and aesthetics of the manual wheelchair. There's a lot of people who could benefit from these, particularly in preventing repetitive stress injuries and pain. Sometimes this can worsen to the point where a power chair is required.
Who Is Appropriate?
- It is well documented that people who self-propel a manual wheelchair, even an appropriately configured ultralightweight MWC, are prone to:
- Repetitive stress injuries
- Shoulders, wrists
- Pain
- This can worsen to the point that mobility is compromised
Other Considerations
- A person who can self-propel, but:
Has upper extremity injury and/or pain
Has decreased cardiopulmonary function
Has decreased strength and endurance
2. A person who can self-propel, but:
Is less efficient in mobility secondary to aging with a disability or aging in general
Is a long-term MWC user who may have lost efficiency
Is a MWC user who cannot manage slopes, varied terrain, and/or long distances without assistance
Powered Options: PAPAWs
- Pushrim-Activated Power Assist (PAPAW)
- Motor in the hub of the wheel
- Motor external to the frame
These PAPAW or pushrim-activated power-assist units are either at the motor, wheel, or external to the frame.

Figure 20. Examples of Pushrim-Actived Power Assist devices.
- How does it work?
- Hybrid system
- Measures force imparted on pushrim and amplifies force through an electromechanical system.
- Amplifies the propulsion phase (faster and increased force)
- Extends the recovery phase (time before another stroke required)
These increase the distance and force of any stroke from the clients.
- So, what exactly does that mean?
- A typical push on the handrim results in more force to propel the MWC further per stroke and with more force up slopes and over varied terrain
- Cool!
It amplifies the propulsion phase or stroke and extends the recovery phase helping a person be more efficient. I am happy to give you more information on that as well.
Resources
- For more information, check out:
- Manual Wheelchair Selection Guide:
- http://www.beneficialdesigns.com/products/pax-press/a-guide-to-wheelchair-selection
- Manual Wheelchair Training Guide:
- http://www.beneficialdesigns.com/products/pax-press/manual-wheelchair-training-guide
- The National Spinal Cord Injury Association Manual Wheelchair information
- http://www.spinalcord.org/resource-center/askus/index.php?pg=kb.page&id=1642
- RESNA Position Paper on The Application of Ultralight Manual Wheelchairs
- http://www.resna.org/sites/default/files/legacy/resources/position-papers/UltraLightweightManualWheelchairs.pdf
- Manual Wheelchair Selection Guide:
I want to thank you for your time today. I know everyone is busy, and I appreciate you putting in the time to continue your education in this area.
Questions and Answers
Are there any effective adaptive equipment options to ease self-propulsion with bariatric wheelchairs?
Some amazingly lightweight bariatric chairs are on the market now. There are a few adjustments that can be made to these frames to ease self-propulsion. However, the reality is at the end of the day, if the wheels are quite a ways away from the client, and the combination of the frame and the client makes for a challenging weight to self-propel. Some bariatric clients, because of that, will end up using power mobility and use the manual as a back-up only.
What type of measurements should be taken from the client to help determine the type of wheelchair for the client, the weight, length of the patient's legs, et cetera?
Several forms guide all the client measurements that need to be taken to best spec out a manual wheelchair. The supplier will often take those measurements as well because they are responsible for fitting the wheelchair. If the chair shows up and is not meeting a client's needs, it is on the supplier. Even if we do our measurements, a good supplier will also typically do their own. Typical measurements include seat depth, seat width, back height, chest width, and some backs and seats can also be a different width depending on the client's needs.
Other measurements include the shoulder to the seat pan, which can help with the back height and the placement of the other components. Much of this depends on seating. Other necessary measurements are from the seat pan to the footplate height and the top of the shoulder to where the elbow is for armrest placement. Components like that are readily adjustable, and we can finalize that armrest height at the time of the fitting. That is another difference with some of these frames. Some of them have a fixed armrest height, and some are adjustable. As I said, some forms out there walk you through some of these particular measurements and things to keep in mind during the evaluation. One resource is a form in Illinois with their Medicaid program. It has been revised many times and is available under Resources on the NRRTS (the National Registry of Rehabilitation Technology Suppliers) website. You can download that form for free or fill it out digitally.
Can one hand and one foot be combined with one hand propulsion style for efficient one-handed self-propulsion?
Yes, if someone is not efficient in one-handed propulsion, they can use one hand and one foot. Again, we have the drawbacks of foot propulsion in that the pelvis is often pulled forward, and the seat floor height is low.
References
Chan, F. H. N., Eshraghi, M., Alhazmi, M. A., & Sawatzky, B. J. (2018) The effect of caster types on global rolling resistance in manual wheelchairs on indoor and outdoor surfaces, Assistive Technology, 30(4), 176-182, DOI: 10.1080/10400435.2017.1307880
Choukou, M. A., Best, K. L., Potvin-Gilbert, M., Routhier, F., Lettre, J., Gamache, S., Borisoff, J. F., & Gagnon, D. (2021). Scoping review of propelling aids for manual wheelchairs. Assistive technology: The official journal of RESNA, 33(2), 72–86. https://doi.org/10.1080/10400435.2019.1595789
DiGiovine, C., & Berner, T. (2018). Alternative drive mechanisms for manual wheelchairs: Bridging the gap between manual and power mobility. In Lange, M. & Minkel, L. (Ed.), Seating and wheeled mobility: A clinical resource guide. Slack Incorporated.
Fitzgerald, Shirley G., et al. "Comparison of fatigue life for 3 types of manual wheelchairs." Archives of physical medicine and rehabilitation 82.10 (2001): 1484-1488.
Gebrosky, B., Bridge, A., O’Donnell, S., Grindle, G. G., Cooper, R., & Cooper, R. A. (2020) Comparing the performance of ultralight folding manual wheelchairs using standardized tests. Disability and Rehabilitation: Assistive Technology. DOI: 10.1080/17483107.2020.1754928
Lange, M. L., & Minkel, J. (2018). Seating and wheeled mobility: A clinical resource guide. Slack Incorporated.
Oliveira, N., Blochlinger, S., Ehrenberg, N., Defosse, T., Forrest, G., Dyson-Hudson, T., & Barrance, P. (2019). Kinematics and pushrim kinetics in adolescents propelling high-strength lightweight and ultra-lightweight manual wheelchairs. Disability and rehabilitation. Assistive technology, 14(3), 209–216. https://doi.org/10.1080/17483107.2017.1417499
Rammer, J. R., Krzak, J. J., Slavens, B. A., Winters, J. M., Riedel, S. A., & Harris, G. F. (2019). Considering Propulsion Pattern in Therapeutic Outcomes for Children Who Use Manual Wheelchairs. Pediatric Physical Therapy: The Official Publication of the Section on Pediatrics of the American Physical Therapy Association, 31(4), 360–368. https://doi.org/10.1097/PEP.0000000000000649
Citation:
Lange, M. (2021). Manual wheelchair mobility: Self-propulsion. PhysicalTherapy.com, Article 4818. Available at www.PhysicalTherapy.com
