Learning Objectives
- Accurately describe at least two examples of the anatomic and bow mechanical relationships of the elbows that relate to normal function.
- Describe without queues the pathomechanics of at least two selected elbow injuries.
- Independently outline an evidenced based examination with at least three intervention techniques for selected elbow conditions.
Anatomy
Articulations
There are three primary articulations: the humeral ulnar, humeral radial, and the proximal radial ulnar joint.
Carrying Angle
Another thing to consider when reviewing anatomy is the carrying angle. There is a normal valgus angulation. In men, that normal angulation ranges between 11 and 14 degrees, and in women, 13 to 16 degrees. The female pelvis is a bit wider which may be a component on why there is a difference in gender. Again, keep in mind the normal position of the elbow is going to have a bit of a valgus angulation.
Ligamentous Complex
Medial ligament complex. The ulnar collateral ligament complex is found on the medial side of the elbow. It has three different bundles. The anterior bundle is going to be taut in extension, the posterior bundle will be taut in flexion, and there is also a transverse bundle. Thickenings of the structure provides some variability in the direction of the fibers, which is going to be more helpful as far as trying to control load.
Restraint to Valgus Stress
Specific literature provides us information regarding restraint to valgus stress and how much each component is contributing. The joint surfaces, or joint articulation will give us some stability, as well as the ligamentous structures and the capsule. How much each is contributing differs a little bit depending on whether or not the elbow is flexed versus extended. You can see those percentages in Figure 1. The joint articulation is giving between 30 and 35% restraint both in elbow flexion and extension. The ligaments are providing a more significant barrier in elbow flexion compared to elbow extension, where as the joint capsule is providing much more restraint in elbow extension compared to elbow flexion.
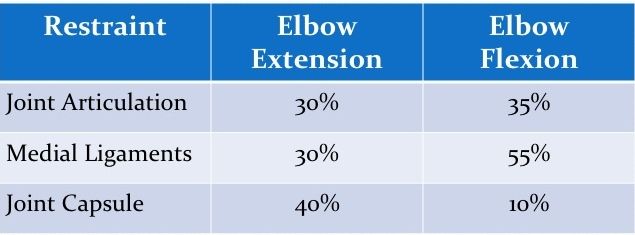
Figure 1. Restraints to Valgus Stress
Lateral Ligament Complex
Looking laterally at the lateral ligament complex:
- Radial Collateral Ligament: taut throughout the entire range of motion.
- Lateral Ulnar Collateral Ligament: primary restraint to varus stress at the elbow.
- Accessory Collateral Ligament: fibers will blend in with the annular ligament.
- Annular Ligament: helps stabilize the proximal radial ulnar joint. The anterior portion of the annular ligament is taut in supination, and the posterior portion is going to be taut in pronation.
Restraint to Varus Stress
Figure 2 displays the percentages for primary restraint to varus stress. Joint articulation provides quite a bit of restraint in both elbow extension and flexion. About 55% restraint is happening with joint articulation and elbow extension. It is as high as 75% when the elbow is flexed. The lateral ligaments and joint capsule are providing about 45% in elbow extension, and only about 10% in elbow flexion. Other soft tissue (the other musculature that's crossing that portion of the joint), doesn't help provide much restraint in elbow extension. Again, elbow extension is going to be our close-packed position, so we're relying on joint articulation, capsular ligamentous structures and extension. There is a small amount of restraint (15%) in elbow flexion. This is more of an open-packed position from the corresponding soft tissues and musculature around the elbow with regard to varus stress.
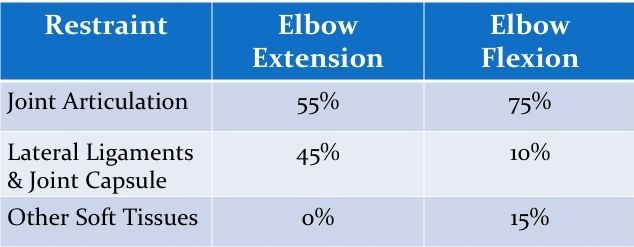
Figure 2. Restraints to Varus Stress
