Editor's note: This text-based course is a transcript of the webinar, Health Literacy in Practice: Effective Communication and Education, presented by Kathleen Weissberg, OTD, OTR/L, CDP, CADDCT, CMDCP, CFPS, CGCS, TIE.
*Please also use the handout with this text course to supplement the material.
Learning Outcomes
After this course, participants will be able to:
- Define health literacy and recognize health literacy concepts including relevant statistics
- Identify appropriate assessment tools to evaluate health literacy levels
- Recognize factors that influence health literacy and describe techniques the practitioner can use to facilitate health literacy in practice
Introduction
Thank you so much for joining me today. This is a topic I feel strongly about, and I am glad you have chosen to spend this time with me exploring it. Health literacy is one of those areas that touches every single patient encounter we have, whether we are in an acute care setting, an outpatient clinic, a skilled nursing facility, or a patient's home. It affects how our patients understand what we tell them, whether they follow through on what we ask them to do, and ultimately, whether the care we provide actually makes a difference in their lives.
In my 30-plus years of practice in rehabilitation and long-term care, I have worked as an executive, researcher, and educator. I currently serve as the National Director of Education for Select Rehabilitation, where I provide continuing education support to over 30,000 therapists, nurses, and administrators nationwide. I am a Certified Alzheimer's Disease and Dementia Care Trainer, a Certified Dementia Care Practitioner, a Certified Montessori Dementia Care Practitioner, a Certified Fall Prevention Specialist, a Certified Geriatric Care Practitioner, and a Trauma-Informed Educator. I also serve as the Region 1 Director for the American Occupational Therapy Association Political Action Committee and as an adjunct professor at Gannon University in Erie, Pennsylvania.
The lens I bring to health literacy is deeply rooted in my experience with older adults in senior living. However, everything we discuss today can be applied across the lifespan and across all practice settings. The skills and strategies I share with you are relevant whether your patients are eight or eighty. My goal today is to give you practical, immediately usable tools that you can take back to your clinical practice. Let us get started.
Definitions
Before we explore the scope and impact of health literacy, it helps to establish a common vocabulary. The terms we use in this course carry specific meaning, and those meanings are worth making explicit from the start.
Literacy, broadly defined, is the ability to understand and use reading, writing, speaking, and other forms of communication as ways to participate in society and achieve one's goals and potential. This includes nonverbal communication. It is, at its core, the capacity to make meaning out of the information we receive and to act on that meaning in the world.
Health literacy is a more specific concept. It refers to the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions. That might mean understanding what a provider is telling you about a diagnosis. It might mean choosing between health insurance plans, navigating a medication regimen, filling out a registration form at a new clinic, or making a follow-up appointment. Health literacy is not simply about whether a person can read. It is about whether they can find, understand, and act on health information in ways that support their own wellbeing.
Health Literacy
Health literacy is shaped by both individual and systemic factors. On the individual side, this includes a person's communication skills, knowledge of health topics, cultural background, and the demands of the specific healthcare situation they are in. On the systemic side, the complexity of the healthcare system itself plays a significant role. How information is presented, how forms are designed, how providers communicate, and what assumptions healthcare environments make about the people they serve all factor in. Both sides of that equation matter, and both are within our scope of influence as therapists and clinicians.
When health literacy is limited, the impacts are real and measurable. Individuals struggle to navigate the healthcare system, complete complex forms, and locate providers or services. They have difficulty sharing their personal health history. They struggle with self-care and chronic disease management. And they face significant barriers around understanding mathematical concepts like probability and risk, which are embedded in medication instructions, dietary guidelines, and nearly every piece of health education material we produce.
Health Literacy Skills
When we think about what health literacy actually requires of a person, two skill categories stand out. The first is numeracy, the ability to work with numbers in a health context. This includes measuring the correct dose of a liquid medication, calculating a deductible or copay, reading a nutrition label, choosing between health plans, and understanding dosage instructions. The second is general health knowledge, the foundational understanding of how the body works, what causes disease, and how diet, exercise, and other lifestyle factors affect health and wellness. Without both of these, individuals cannot reliably manage their own health.
This is not just a challenge we face in the United States. Limited health literacy is a global crisis. And here is the practical reality we all need to sit with: without clear communication on our end, we cannot reasonably expect the people we serve to adopt the healthy behaviors, home programs, and self-management strategies we promote. If we hand someone a discharge packet filled with jargon and paragraph after paragraph of dense text, we should not be surprised when they do not follow through.
Plain Language
The answer to that communication gap, in large part, is plain language. Plain language is communication that a reader can understand the first time they read or hear it, with reasonable time and effort. A plain language document is one in which individuals can find the information they need, understand it, and act on it appropriately. Note that last piece: act on it. Plain language is not just about simplicity for its own sake. It is about enabling action.
The key elements of plain language include organizing information so that the most important points come first, breaking complex information into understandable chunks, using simple language and defining technical terms, and writing in the active voice. I think sometimes in therapy we try to give patients everything they would ever need to know about their diagnosis in a single handout. Sometimes less is more. Let us put the critical information at the top. Let us break it into pieces that they can process. Let us make sure the language we use is plain, not just to us, but to them. What is plain to a physical therapist with a doctoral degree is not necessarily plain to a retired coal miner or a first-generation immigrant.
Key Statistics and Findings
The statistics around health literacy are sobering, and I want you to sit with them for a moment because they have direct implications for every patient we see.
Only 12% of U.S. adults have proficient health literacy. Let that sink in. That comes from the National Assessment of Adult Literacy, and it represents a widespread, systemic struggle. Roughly 36% of adults have basic or below-basic health literacy, meaning they will struggle to understand a drug label, their medication's side effects, appointment instructions, or basic written health communications. The economic impact is staggering: costs associated with limited health literacy are estimated at $349 billion annually in the United States alone. And the health correlation is stark: 42% of individuals with low or limited health literacy rate their own health as poor.
Here is a statistic that I find particularly striking. Anywhere between 48 and 59 million adults in the U.S. read below a third-grade level. Just a few years ago, that number was approximately 36 million. It has since grown to nearly 60 million. That shift represents a meaningful, measurable change in the population we serve, and we need to respond accordingly.
Key Vulnerable Groups
Although limited health literacy can and does affect adults of all ages, backgrounds, and education levels at some point in their lives, certain groups face disproportionately higher rates and more severe consequences.
Older adults aged 65 and older are particularly vulnerable. As individuals age, they often experience cognitive and sensory changes, as well as a generational distance from formal education, which can make processing complex health information more difficult. In my experience in senior living, some of our residents completed their formal education many decades ago. What they learned may no longer reflect current evidence, and they may not have had ongoing opportunities to develop health-specific knowledge and skills.
Socioeconomic factors are also strongly predictive. Low income, low educational attainment, less than a high school diploma, and systemic poverty are all associated with limited health literacy. Racial and ethnic disparities exist as well: Black, Latino, and American Indian and Alaska Native populations face disproportionately higher rates of limited health literacy than other groups. This connects directly to why immigrants and individuals with Limited English Proficiency (LEP) are also significantly impacted. We will discuss language assistance strategies later in this course.
Insurance status is another factor that emerged clearly in the research I reviewed. Individuals on Medicaid, Medicare, or who are uninsured are more dramatically affected. This has obvious relevance for the populations many of us serve in skilled nursing, post-acute, and home health settings. Individuals with chronic diseases such as hypertension, type 2 diabetes, COPD, and congestive heart failure, as well as those with disabilities or compromised health, also face elevated risk. Finally, rural populations also show higher rates of limited health literacy.
I want to be clear about what I mean when I say these groups are vulnerable. I do not mean that all of these individuals have limited health literacy. I mean, there is a higher likelihood that health literacy challenges may exist, and that likelihood should inform how we approach every clinical interaction.
Incidence and Identification
Nearly nine out of every ten people in the United States have limited health literacy. Read that again: nine out of ten. That is 90 percent.
And here is something I want to underscore, because it surprises many clinicians the first time they hear it: education level is not a reliable predictor of health literacy. I think about my own parents, both college-educated, successful in their careers, now in their mid-eighties. When things arrive in the mail related to Medicare, prescription renewals, or forms they need to fill out, they are frequently unsure what to do. Education, particularly formal education completed decades ago, does not guarantee health literacy.
Because the prevalence is so high and the predictors are so unreliable, the Agency for Healthcare Research and Quality (AHRQ) recommends that we approach health literacy with what they call universal precautions. Just as we apply standard precautions in infection control to protect every patient regardless of their known disease status, universal precautions for health literacy means assuming that most individuals will struggle to understand health information and designing all of our communications accordingly. We write and speak at a level that everyone can access, roughly a sixth-grade reading level or below. If I give a person with high health literacy materials designed for lower literacy, they are not going to be offended. But if I give a person with limited health literacy materials that are too complex, I have failed them.
Signs of Low Literacy
Knowing how to recognize the signs of low literacy in a clinical encounter is essential, as individuals with limited reading ability work hard to hide it. There is real shame and stigma associated with literacy challenges, and many patients will go to considerable lengths to avoid being identified.
Some of the most telling behavioral signs relate to medication management. A patient may not know the names of their regularly used medications. They may not be able to explain a medication's purpose or their dosing schedule. I have watched this with my own parents: they identify their medications by how they look, not by reading the label. They pick up the blue oval one or the small white round one. I find myself wondering, what happens if the generic version looks completely different from the brand name?
Other behavioral signs include poor compliance with treatments and appointments, frequent missed appointments, failure to follow through on lab tests or referrals, and watching and mimicking others rather than following written instructions. Patients may bring a family member to every appointment, not because they want to involve them, but because they need someone who can read for them. They may ask fewer questions or offer deflective responses to written information: "I forgot my glasses, I will read this when I get home," or "Let me take this home to discuss with my kids." Registration forms may come back incomplete or contain errors.
None of these behaviors, on their own, is definitive proof of limited literacy. But when we notice patterns, we need to respond thoughtfully and without shaming the individual. Our role is to create an environment where the person feels safe, supported, and able to ask for the help they need.
Key Impacts on Health Outcomes
Limited health literacy does not just affect how well someone understands a pamphlet. It is linked to measurable, significant impacts on health outcomes.
The first and most foundational is a worsened health status. Limited health literacy is strongly associated with poor self-rated health, particularly for individuals with chronic diseases. It also reduces a person's ability to manage those diseases, to engage in self-care, and to maintain their own health and wellness over time. These individuals are less able to follow a home exercise program, manage a medication regimen, or monitor their own vital signs at home.
From there, we see increased healthcare utilization, particularly more emergency department visits and longer hospital stays. People with limited health literacy tend to delay seeking care until a situation becomes serious, which means they are more likely to end up in the ER than to have a proactive wellness visit. Related to this, we see reduced preventive care: fewer screenings, fewer routine check-ups, fewer pap smears or mammograms. Chronic diseases go undetected longer. Risks accumulate.
Poor treatment adherence follows logically. If someone does not understand their medication instructions, whether a drug should be taken on an empty stomach, at a specific time of day, or avoided with certain foods, they cannot follow them correctly. I have seen individuals who were genuinely trying to comply with their regimen, but the information they were given was simply beyond their ability to process and use.
Ultimately, limited health literacy is associated with advanced illness at the time of diagnosis, delayed treatment, and higher mortality. Much of this traces back to a single root cause: misunderstanding health information. Individuals may misinterpret a message from their care team. They may not know how to log in to a patient portal, access a MyChart message, or know what to do when a prescription needs to be refilled. Barriers accumulate, care is delayed, and outcomes suffer.
Stigma and Shame
One impact I want to address specifically is the psychological and emotional dimension of low health literacy, which is often overlooked and profoundly shapes how we approach our patients.
Low health literacy carries significant stigma. Individuals who struggle with reading or processing health information are very often aware of it, and they feel shame about it. They work hard, sometimes extraordinarily hard, to conceal their difficulties. The goal is to maintain their dignity. And as practitioners, we need to be deeply cognizant of this.
In practice, this means that a patient who is nodding along during our instruction may not understand anything we are saying. A patient who says, "Yes, I understand," may be saying it because understanding is expected of them, not because they actually understand. A patient who hands back an incomplete form may be protecting themselves from having to explain why they could not complete it. Our role is to create interactions that are shame-free, that invite questions, and that normalize the process of checking for understanding without making the individual feel exposed or embarrassed.
Role in Senior Living
One of the overarching goals articulated in both Healthy People 2020 and Healthy People 2030 was to eliminate health disparities, achieve health equity, and improve the health and well-being of all people. Health literacy is central to that mission, and we, as therapists and clinicians, have a meaningful role to play.
In senior living specifically, this role is clear: we ensure that any health-related information or education we provide aligns with the person's literacy abilities, cultural sensitivities, and verbal, cognitive, and social skills. We provide information and education that promotes self-management for optimal health and participation. And we facilitate health literacy at the systems level by promoting environments and care processes that align with health literacy principles.
Across all settings, this means being informed, being aware, and being deliberate. We cannot assume that a patient who nods their head or smiles has understood what we said. We cannot assume that a patient who appears engaged during a therapy session will be able to reproduce our instructions at home. And we need to recognize the barriers our patients bring with them: functional declines associated with aging, limited formal education, different native languages and cultural beliefs, disabilities, and experiences in early childhood that may have included trauma or educational disruption.
Integrating Health Literacy into Practice
The first practical step in integrating health literacy into practice is making information accessible, and that means a lot more than handing someone a sheet of paper. It means adapting information to individual needs, circumstances, and abilities. It means communicating comprehensively across multiple channels. Oral instructions alone are not enough. Written materials alone are not enough. Combining the two, and adding demonstration, experimentation, and repetition, gives your patients the best chance of actually learning and retaining what you are teaching.
When we give someone a home program or any written instruction, we want the document to be written in the active voice, using clear, simple language. Pictures and drawings help illustrate procedures. Interactive elements and recaps reinforce the message. The most important information should come first, and the material should be personalized so it feels relevant to the individual's own life and situation.
When we communicate orally, a structured approach helps. I get the person's attention first. I make eye contact. I announce the subject: here is what we will be talking about today. I convey the message clearly and concisely. And then I ask the person to tell me back, in their own words, what they heard.
Ask Me
One of the tools I weave into this process is Ask Me 3, which invites the client to engage around three core questions:
- What is your main problem today?
- What do I need to do for you concerning this problem?
- Why is it important to you?
This reframes the encounter so the individual is a participant rather than a passive recipient, and it helps me develop genuinely patient-centered goals. It also creates a shame-free environment where asking questions is normalized.
We also need to recognize that individuals who have low health literacy are reluctant to ask questions. They are often skillful at concealing their challenges. That is where we need to ask more questions, ask them to demonstrate, and be certain they understand what we are communicating. We need to identify each person's characteristics: their knowledge level, teaching preferences, skills, beliefs, and any cultural barriers.
Finally, I want to address the importance of not overburdening our patients with information. I have a discharge packet on my desk right now from a recent family member's hospital visit. It is ten pages long, and some of it does not even apply to that individual's situation. When we send someone home with materials, we should ask: What are the three to five things this person absolutely must know and do? What is critical? Breaking information into essentials, organizing it clearly, and following up afterward to ensure recommendations are implemented are all core elements of effective health literacy practice. We also want to increase our own cultural competency, involve the family, and follow up on interventions to confirm that recommendations are being followed and that the patient has no remaining questions.
Effective Communication with Diverse Populations
Communication
Research clearly demonstrates that communication quality directly affects patient outcomes (Muñoz & Luckmann, 2005). Compared to patients who are simply told what to do, those who are encouraged to discuss their perceptions of illness and expectations for treatment experience a greater sense of control, feel more involved in their care, suffer less anxiety, and are more likely to accept treatment schedules and follow through on recommendations. In short, patients who are partners in their care do better than those who are passive recipients.
When we have patients or clients who speak a different language than we do, or who have limited English proficiency, the quality of that communication partnership is at risk. This is where language assistance services become essential, both legally and clinically.
Overview
Interpretation and translation are two very different things. Interpretation is the process of conveying verbal or signed communication in real time. Translation is the conversion of written documents from one language to another. Both are important, and both require expertise. A bilingual coworker is not a trained interpreter. A quick pass through an online translation tool is not the same as a professionally translated and back-translated document.
Using interpreter services and translated documents ensures better understanding by providing a common language. Language assistance services help us provide quality care to all patients by facilitating effective communication across linguistic barriers.
With Language Assistance
With appropriate language assistance in place, patients are more likely to understand their health conditions and treatment plans, to follow health recommendations, and to rate their care positively. The investment in language access is not just an ethical obligation; it is a clinical quality issue. This is a point I feel strongly about: our patients have a right to understand the care we are providing, and we have a professional obligation to make that possible, regardless of the language they speak.
Language Assistance Services
Formal language assistance services encompass trained interpreters who are fluent in both the provider's language and the patient's language, translated written materials such as intake forms, consent documents, and patient education materials, and graphic materials and signage that can communicate across language barriers.
Interpretation services are provided specifically for individuals with limited English proficiency and for those whose primary communication mode is American Sign Language. A trained interpreter in a healthcare setting is performing a complex, demanding task, and the quality of that interpretation directly affects the quality of care. Appropriate use of trained interpreters is not optional for individuals with LEP; it is a legal right.
Interpreter Services
Interpretation is defined as the process of understanding and analyzing a spoken or signed message and re-expressing that message faithfully, accurately, and objectively in another language, taking the cultural and social context into account. This is a high-skill task, and it is critically different from simply being bilingual. A trained medical interpreter understands clinical terminology, recognizes the limits of their role, and knows how to navigate the cultural nuances that arise in healthcare conversations.
Providing Written Materials
Written materials are an important adjunct to oral communication, not a substitute for it. Translated written materials may include signage, intake applications, consent forms, and medical, treatment, and exercise instructions. When determining what should be translated and for whom, the first step is to clearly identify the audience: their literacy level, language, dialect, and culture.
The gold standard for translation is back-translation, a process in which materials are translated from English into the target language by one person and then translated back into English by an independent person. The two English versions are then compared to confirm that the message has been preserved accurately. In our own organization, we use this process for all materials we translate into Spanish, and it has caught meaningful errors that would otherwise have gone out to patients and families.
Obtaining Translated Materials
When a professional translator or translation service is not immediately available, there are resources. Using trained, internal bilingual staff members as translators is one option. Hiring a translation company provides professional accountability. Collaborating with members of the target community is particularly valuable for capturing dialectical and cultural nuances that a general translation might miss. Organizations can also purchase pre-translated materials, locate web-based resources, or research resources available through state Medicaid programs, insurance companies, or pharmaceutical companies. Whatever the source, materials should be evaluated before distribution to confirm they communicate the intended message accurately.
Involve the Community
Involving the community being served in the development and review of translated materials ensures those materials meet community needs, reflect differences in dialect and culture, and are appropriate for the community's level of education, culture, and literacy. This step is often skipped in the interest of time, but it is one of the most effective quality checks available and results in materials that patients will actually understand and use.
Use of Symbols
When language barriers cannot be fully bridged through words alone, visual communication tools become invaluable. Universal healthcare symbols, such as those developed through the Robert Wood Johnson Foundation's Hablamos Juntos program, offer a shared visual vocabulary that transcends language. Many of these symbols are already familiar to patients from everyday signage and are easily interpreted. Using these symbols in clinic spaces, educational materials, and patient communications can meaningfully reduce confusion for patients with limited English.
Posting signage in multiple languages that informs patients of their right to an interpreter is both a legal best practice and a practical health literacy strategy.
Figure 1: Sample of Universal Healthcare Symbols from Hablamos Juntos with support from the Robert Wood Johnson Foundation

Image: Society for Environmental Graphic Design at https://cdn.segd.org/wp-content/uploads/2024/12/14_SEGD_Universal-Symbols-for-Healthcare.pdf) before final publication.
Graphic Cards
Graphic cards are another practical communication tool, particularly for patients who have limited literacy or limited English proficiency. The Wong-Baker FACES Pain Rating Scale is widely recognized and bridges the language barrier in pain assessment with a set of facial expressions that most patients can interpret intuitively. Tools like this allow us to gather meaningful clinical information without relying on complex verbal or written communication.
Figure 2: Wong-Baker FACES Pain Rating Scale
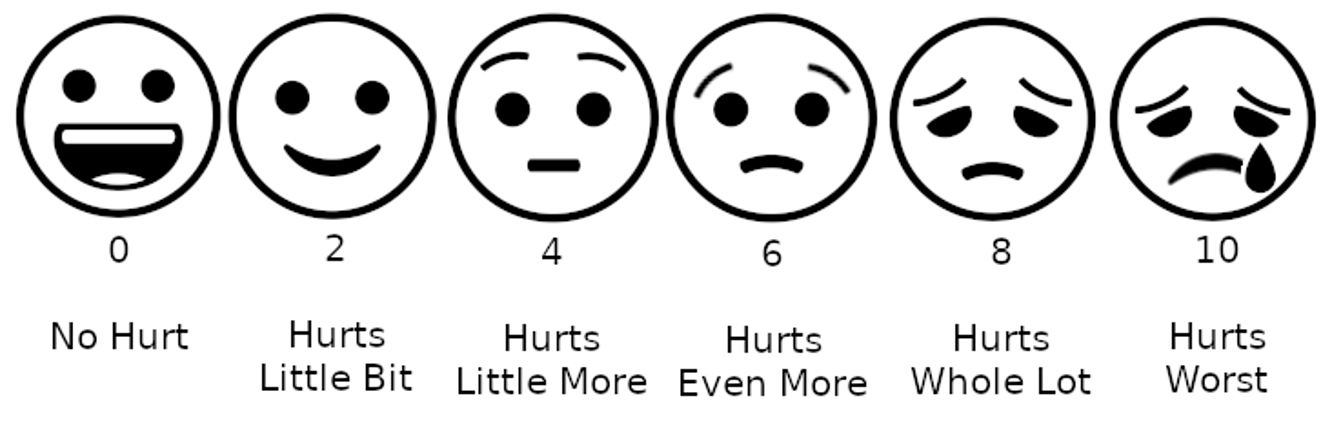
Image: Belbury, CC BY-SA 4.0, via Wikimedia Commons) before final publication.
Obtaining Translated Materials
If written materials cannot be created in the original language, there are many options for obtaining translated materials, including:
- Using trained, internal bilingual staff members as translators,
- Hiring translation companies,
- Collaborating with the community of the target audience,
- Purchasing translated materials,
- Locating web-based resources, and
- Researching other resources, such as state Medicaid programs or insurance companies, which may provide patient education materials in a variety of languages.
Whatever the source of the written materials, it is important that they be evaluated to make certain they correctly state the health information they are intended to provide and that they are appropriate for the intended audience’s literacy level, culture, and language.
Involve the Community
Involving community members in developing and reviewing translated materials can help to ensure that the materials:
- Meet community needs,
- Reflect differences in dialect and culture, and
- Are appropriate for the community’s cultures, education, and literacy levels
- Are accurate and useful and accurately reflect patients' cultures and lifestyles.
Figure 3: Signage for Right to Interpreter
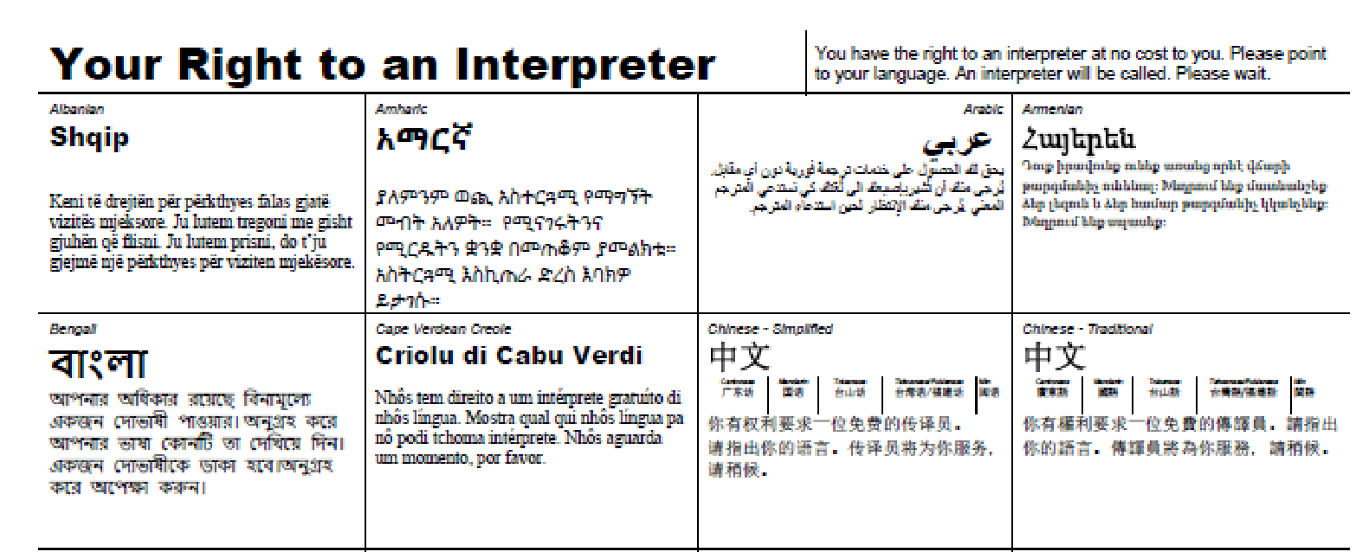
Image: NC Department of Environmental Quality
I Speak Cards
"I Speak" cards, which allow patients to point to their primary language and request interpretation, are another practical resource. These cards are available from organizations such as the DC Office of Human Rights and can be kept readily available at reception desks, therapy gyms, and nursing stations to support immediate language identification.
Figure 4: I Speak Cards Example in English
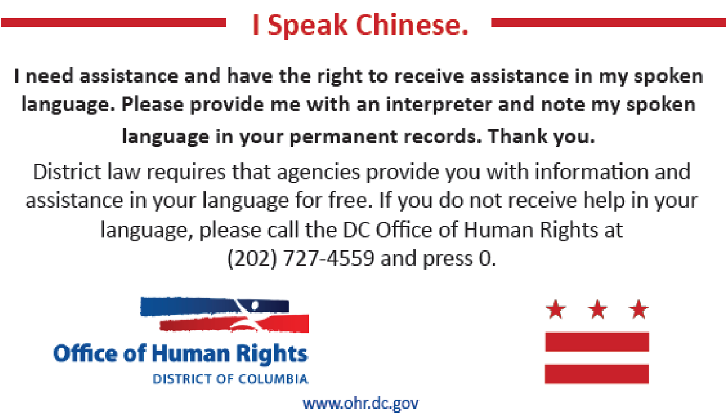
Figure 5: I Speak Cards Example in Native Language (Chinese in this case) on the Opposite Side of the Above Card
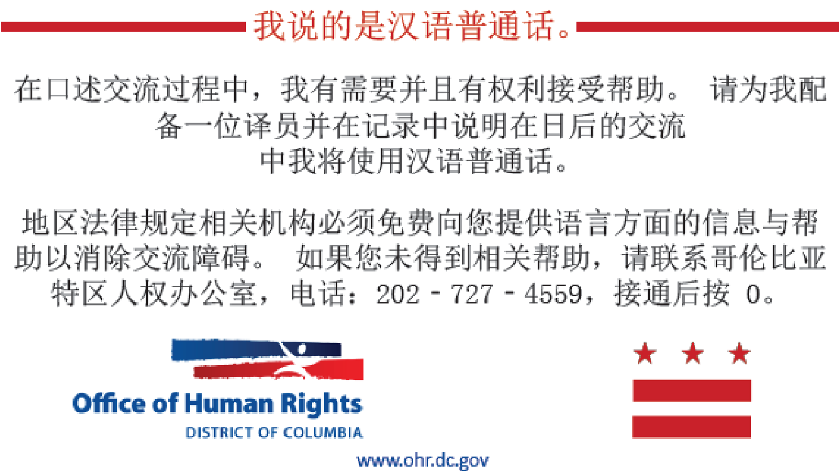
Image: Office of Human Rights
Interpreter Roles
There are three main roles of an interpreter:
- Conduit: This is the most basic interpreter role (default role). The interpreter conveys verbatim in the target language what has been said by the other in the source language, without additions, omissions, editing, or polishing.
- Culture Broker: The interpreter provides a necessary cultural framework for understanding the message being interpreted.
- Clarifier: The interpreter explains or makes word pictures of terms that have no linguistic equivalent (or whose linguistic equivalent will not be understood by the patient) and checks for understanding.
In a health care setting, the preferred role for an interpreter is normally that of a conduit, which is the most basic role.
Triadic Interview
When working with an interpreter in a clinical encounter, the structure of the interaction matters. A triadic interview involves three parties: you, the patient, and the interpreter. The key principles are straightforward but easy to overlook. Face the patient, not the interpreter. Speak directly to the patient, using second-person language: "How are you feeling?" not "Ask her how she is feeling." The interpreter should remain as unobtrusive as possible. Before the session, take a few minutes to meet with the interpreter, explain the purpose of the visit, and establish ground rules for their role.
A few additional best practices for interpreter-assisted sessions
- Insist on sentence-by-sentence interpretation rather than allowing long passages to accumulate before being conveyed
- Explain clearly that the interpreter is not to answer for the patient
- Invite the interpreter to interject if clarification becomes necessary
- Document the interpreter's name in your clinical notes
- Give the interpreter a brief summary of the patient and, together, establish session goals
- Allow the interpreter to ask open-ended questions to clarify the patient's statements
- Speak slowly and clearly, use simple and straightforward language, avoid metaphors and idioms, and explain any medical terminology you use
- Allow time for the patient to ask questions
- Verify understanding by asking the patient to repeat back key information in their own words, and
- Be aware of your own attitudes and any biases you may bring to the interaction.
Readability Tools
Did you know that 75 out of 100 Americans can read at a sixth-grade level without difficulty? A fourth to sixth-grade readability level is accessible to most adults. A seventh to eighth-grade level is accessible to about half or more. High school level and above is accessible to relatively few adults. So if we are producing materials at a reading level above that of a fifth- or sixth-grader, we are already narrowing our audience considerably. The question is: how do we know where our materials land?
Clinician Role
We need to provide health education to our clients. We must be mindful of their literacy skills, including reading ability and comprehension. We can formally assess reading ability. We can also informally discuss with clients their previous level of schooling, educational achievement, and perceived reading ability. Both approaches provide information we can use to calibrate our communication and materials. The goal is not to make the patient feel evaluated or embarrassed. The goal is to ensure that everything we produce and say is accessible to the individual sitting in front of us.
Fry Readability Formula
The Fry Readability Formula has been around for many years and is one of the most straightforward tools available. You select a passage of text, run it through the formula, and it assigns an approximate grade-level reading score based on the vocabulary and sentence structure of the text rather than the organization or content. The grade-level reading is determined by plotting the average number of sentences and syllables from three 100-word passages on a graph. The graph measures reading levels from first grade through college. You can access the Fry formula through several free online tools, and it is a reliable first pass for any patient education material you are developing.
Flesch-Kincaid Grade Level Readability Formula
The Flesch-Kincaid Grade Level Readability Formula is perhaps the most widely used readability tool in healthcare and patient education. Available at www.readabilityformulas.com, it uses seven different popular readability formulas to calculate an average grade level, reading age, and text difficulty score for a sample of text. It is considered one of the oldest and most reliable readability formulas available.
To illustrate just how important readability is in real clinical materials, I want to share an example. I encountered a handout being distributed to patients preparing for hip replacement surgery at a well-known California hospital. The materials read as follows: "The rate of medical complications following hip replacement surgery is extremely low. Serious infections, such as a hip joint infection, occur in less than 2 percent of patients. The most common cause of infection occurs when bacteria enter the bloodstream during dental procedures, urinary tract infections or skin infections". When tested with the Flesch-Kincaid, this passage scores at the 11th-grade reading level. That is the standard we are holding our patients to when we hand them this information in the clinic.
Here is a rewritten version of the same content: "Most people who have hip surgery have less pain. They can get back to doing things they need to do -- like getting dressed, bathing, and walking. After surgery, you will not be allowed to do certain things like play certain sports or jog. Before surgery, you need to see your doctor who will tell you if surgery is safe for you." This version scores at a 5th-grade reading level, and it communicates the essential information clearly and accessibly. That is the difference plain language makes.
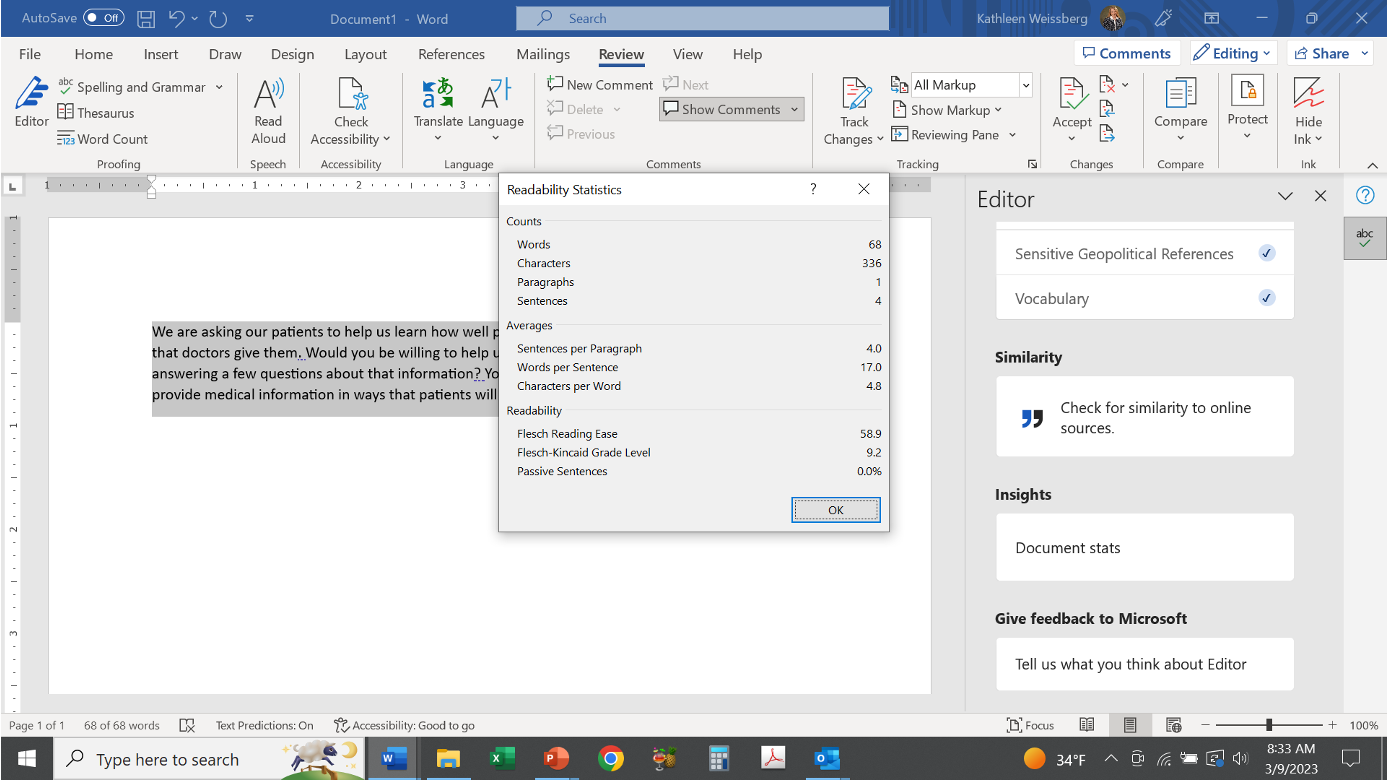
Microsoft Word
You do not need a third-party tool to check your readability. Microsoft Word includes a built-in feature that calculates readability statistics for any document. To access it, go to the Review tab, select Editor, and then choose Document Stats from the Insights section. You will receive comprehensive counts of words, characters, paragraphs, and sentences, along with averages for sentences per paragraph, words per sentence, and characters per word. Most importantly, it will give you a Flesch Reading Ease score, a Flesch-Kincaid Grade Level, and information about passive sentence use.
Figure 6: Microsoft Word Readability Statistics Feature
Figure 7: Microsoft Word Readability Statistics Dialog Box
I use this tool regularly when I put together materials for our patients and teams. Any time I am developing a newsletter, a home program, or an educational handout, I run it through the readability checker before it goes out. It is a simple habit that takes less than a minute and makes a significant difference in accessibility.
Health Literacy Assessment Tools
Now, let us shift from assessing our materials to assessing our patients. Several validated tools are available to assess an individual's health literacy. Knowing where a patient falls on the health literacy spectrum allows us to tailor our communication, education methods, and materials to meet their specific needs.
Test of Functional Health Literacy in Adults (TOFHLA)
The Test of Functional Health Literacy in Adults (TOFHLA), developed by Parker and colleagues in 1995, is a comprehensive tool that measures functional literacy using real-life healthcare materials. The full version contains 67 items, including 17 numeracy items and 50 reading comprehension items, and takes approximately 22 to 25 minutes to administer. The assessment materials reflect actual clinical contexts: prescription bottle labels, appointment slips, Medicaid applications, informed consent documents, and patient education materials. This is what I mean by functional literacy. It is not about reading a passage in isolation. It is about navigating the actual documents our patients encounter every day.
There are two additional versions of the TOFHLA worth knowing. The TOFHLA-S is a Spanish translation of the full tool. The S-TOFHLA is a shortened version that retains the same constructs and takes approximately seven minutes to complete. In practice, the S-TOFHLA is the version I tend to gravitate toward. Seven minutes is not a significant imposition on either the clinician or the patient, and it provides a reliable snapshot of the individual's functional health literacy.
Rapid Estimate of Adult Literacy in Medicine—Short Form (REALM-SF)
The REALM-SF is one of my favorite tools because it is beautifully simple. Developed by Andrus and Roth (2002) as a short form of the original 66-item REALM instrument, this seven-item word recognition test provides a quick assessment of health literacy in one to two minutes. You hand the patient a card with seven words printed on it and ask them to read each one aloud: behavior, exercise, menopause, rectal, antibiotics, anemia, and jaundice. That is it. It has been validated and field-tested with excellent agreement with the full 66-item REALM instrument.
The scoring is equally straightforward. If a patient reads none of the words correctly, they are functioning at roughly a third-grade level or below, meaning they will not be able to read even most low-literacy materials. They will need oral instruction, and you should consider video, audio, photographs, or illustrations to communicate your clinical content. A score of 1 to 3 places them at a fourth- to sixth-grade level: they can manage low-literacy materials but may not be able to read prescription labels reliably. A score of four to six places them at a seventh to eighth-grade level: they will struggle with some patient education materials, though they will generally not be offended if you give them low-literacy versions. A score of seven places them at high school level or above, meaning they should be able to read most patient education materials.
This goes back to that principle of universal precautions. We should probably be designing everything in a low-literacy mode. It will not offend people who have higher literacy, and it will genuinely help a large portion of the individuals we serve. The REALM-SF simply tells us with more precision where any given individual falls on that spectrum, so we can calibrate our approach.
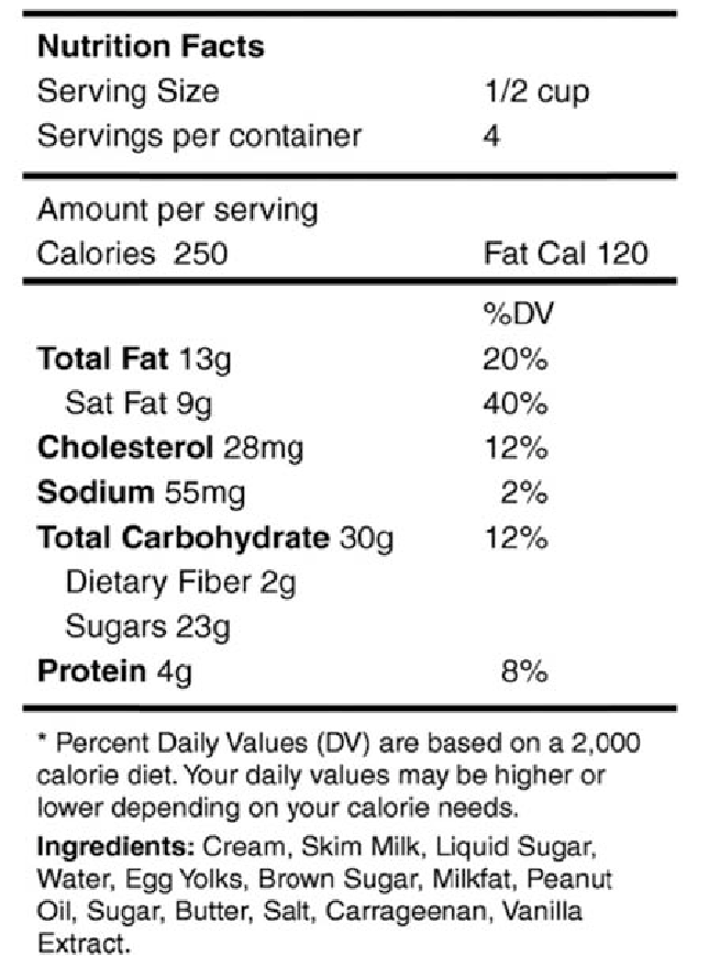
The Newest Vital Sign
The Newest Vital Sign (NVS), developed by Pfizer in 2016, is an elegant tool that assesses health literacy in approximately three minutes by asking the patient to interpret an ice cream nutrition label. It is called the Newest Vital Sign because the recommendation is to administer it at the same time as other vital signs are taken, making health literacy screening a routine part of every patient encounter, not an afterthought.
Why an Ice Cream Label?
I always get a few curious looks when I explain this, so let me take a moment to describe the logic. Analyzing a nutrition label requires the same skills as understanding medical instructions. It requires prose literacy, which is the understanding and application of words in context. It requires numeracy, which is the ability to work with numbers and make calculations. And it requires document literacy, which is the ability to navigate a formatted document and use that information to make decisions. Whether you are reading a nutrition label or a medication instruction sheet, you need to remember numbers, make calculations, identify potentially harmful content, and make decisions based on the information. The ice cream label tests all three of those skill domains in a single, compact, and non-threatening task.
Prose Literacy Example. Clinical example: The patient has scheduled some blood tests and is instructed in writing to fast the night before the tests. Ice cream label example: The patient needs this skill to read the label and determine if he can eat the ice cream if he is allergic to peanuts.
Numeracy Example. Clinical example: A patient is given a prescription for a new medication that needs to be taken at a certain dosage twice a day. Ice cream label example: The patient needs this same skill to calculate how many calories are in a serving of ice cream.
Document Literacy Example. Clinical example: The patient is told to buy a glucose meter and use it 30 minutes before each meal and before going to bed. If the number is higher than 200, he should call the office. Ice cream label example: The patient needs this skill to identify the amount of saturated fat in a serving of ice cream and how it will affect his daily diet if he doesn’t eat it.
Figure 8: Newest Vital Sign Ice Cream Nutrition Label
Administration. To administer the Newest Vital Sign, I recommend the following standardized introduction: "We are asking our patients to help us learn how well patients can understand the medical information that doctors give them. Would you be willing to help us by looking at some health information and then answering a few questions about that information? Your answers will help our doctors learn how to provide medical information in ways that patients will understand. It will only take about 3 minutes".
You hand the nutrition label to the patient, allow them to hold it, and refer back to it throughout the assessment. There are six questions, administered in sequence. You give the patient as much time as they need. If they are struggling significantly with the first or second question after two to three minutes, it is likely they have limited health literacy, and you can stop the assessment at that point.
A few important administration rules: do not prompt the patient toward a correct answer; do not show them the score sheet; and do not tell them whether their answers are correct or incorrect until the assessment is complete. If they get question five incorrect, do not ask question six. If they get four correct answers, you can stop, as adequate literacy has been established.
The six questions and their correct answers are: (
- 1) If you eat the entire container, how many calories will you eat? Correct answer: 1,000.
- (2) If you are allowed to eat 60 grams of carbohydrates as a snack, how much ice cream could you have? Correct answer: one cup, or any amount up to one cup.
- (3) Your doctor advises you to reduce saturated fat. You usually have 42 grams each day, including one serving of ice cream. If you stop eating the ice cream, how many grams of saturated fat would you be consuming? Correct answer: 33 grams.
- (4) If you usually eat 2,500 calories per day, what percentage of your daily value of calories will you be eating if you eat one serving? Correct answer: 10 percent.
- (5) Pretend you are allergic to penicillin, peanuts, latex gloves, and bee stings. Is it safe for you to eat this ice cream? Correct answer: No.
- (6) Why not? Correct answer: Because it contains peanut oil.
The scoring is as follows: a score of 0 to 1 indicates a high likelihood (50 percent or more) of limited literacy. A score of 2 to 3 indicates a possibility of limited literacy. A score of 4 to 6 indicates adequate literacy.
The following table summarizes the major health literacy assessment tools discussed in this course:
Table 1: Comparison of Health Literacy Assessment Tools
| Assessment | Administration Time | Measures |
|---|---|---|
| TOFHLA (Parker et al., 1995) | 22-25 minutes | Numeracy and reading comprehension using real-life healthcare materials |
| S-TOFHLA (Parker et al., 1995) | 7 minutes | Same as TOFHLA, shortened format |
| REALM (Andrus & Roth, 2002) | 1-2 minutes | Medical word recognition does not assess reading comprehension |
| Newest Vital Sign (Pfizer, 2016) | 3 minutes | Numeracy and reading comprehension using an ice cream nutrition label |
Effective Verbal and Written Communication
Ask Me 3
One of the tools I use regularly and recommend wholeheartedly is Ask Me 3. Originally developed as a patient empowerment tool, Ask Me 3 is intended to help patients become more active members of their healthcare team. It centers the clinical encounter around three questions that the patient should be able to answer:
- What is my main problem?
- What do I need to do?
- And why is it important for me to do this?
In practice, this reframes the encounter in a way that is deeply meaningful for the person sitting across from me. It reduces the power differential. It invites them into a conversation rather than making them the passive recipient of instructions. It helps me develop goals that are genuinely patient-centered because I ask the patient what matters to them rather than assuming I already know. It also creates a shame-free environment where asking questions is normalized and encouraged. Encouraging clients to ask questions and taking an understanding attitude are core to making this tool work in practice.
Teach Back
Teach-back is a strategy that should be part of every clinician's toolkit. The concept is simple: after providing instruction or information, you ask the client to repeat what they understood in their own words. You might say, "Can you show me how you are going to do your exercises?" or "Tell me how you will work this into your day." The goal is not to quiz them, and it should never feel like a test. The goal is to assess your own communication effectiveness.
This is a critical distinction: if the person cannot teach it back, that is not primarily their failure. It is a signal that my communication needs work. I need to rephrase, demonstrate differently, simplify, or try a different modality entirely. The teach-back puts the responsibility for clear communication squarely where it belongs: on us as practitioners.
Content and Organization
When creating written materials for patients, content and organization are the foundation. The purpose of the material should be immediately evident to the reader. Do not bury the key message in the middle of a page. Put it first. Make sure the content is balanced, accurate, and current, and include a publication or revision date on all materials. In healthcare, information becomes outdated quickly. A home program written two years ago may contain guidance that is no longer consistent with current evidence.
Every piece of material you create should provide how-to information relevant to the reader's specific situation. Use subheadings, question-and-answer formats, bullet points, and summaries to structure content so it is easy to scan and navigate. Where we consistently fall short is in producing documents that are full of undifferentiated paragraphs. That format is genuinely challenging for most readers, regardless of their literacy level. Breaking information into clearly labeled sections makes it more accessible for everyone.
Layout and Illustrations
Layout choices significantly affect readability. Use ample white space: text-heavy, dense pages are harder to process than those with visual breathing room. You can add white space by using shorter paragraphs, wider margins, and graphic elements that break up the text.
Use serif typefaces, such as Times New Roman, with a minimum font size of 12 points. Serifs, the small horizontal strokes at the base of characters, improve readability in printed text. Avoid fancy or script fonts. Avoid capitalizing all letters in a word, using excessive italics, or using Roman numerals. When you include illustrations, place them next to the text they accompany, not on the following page. Label all illustrations clearly. And make sure your illustrations are culturally appropriate and actually augment the message. Decorative clip art that does not connect to the content undermines the material's purpose. If you include photographs or drawings, make sure they are relevant to the document's content.
Good contrast between text and background is essential. Black text on a white background remains the gold standard. White text on a dark background, while visually striking, is more difficult to read for most people.
Writing Tips for All Readers
Plain writing principles are straightforward, and they apply whether you are writing a home program, a discharge summary for the patient's file, or an educational flyer for your waiting room. Use plain English. Make every word count. Be clear and brief. Use positive words. Use short lists or bullet points rather than long run-on sentences. Choose concrete, familiar words. Aim for one or two syllables per word when possible.
Follow standard grammar conventions: keep the subject and verb close together in a sentence, use vivid and active verbs, write in the active voice, and use short and simple sentence structures. Use personal pronouns such as "you" and "your" to make the material feel relevant to the specific reader. Limit the use of present participle constructions with "-ing" and avoid excessive prepositional phrases, both of which add length without adding clarity.
Your target reading level for most patient materials is fifth- to sixth-grade. Use clear, simple, and common language. Avoid jargon, and define any specialist terminology you must use. If you write the words "range of motion" or "activities of daily living" in a patient document, explain what those terms mean. Do not assume that because these phrases are part of your daily vocabulary, they are part of your patients' daily vocabulary. Write in the active voice and in the second person to keep the reader engaged and the message direct.
Text Appearance Matters
Text formatting is not simply an aesthetic choice. It directly affects how readable and accessible a document is for your patients. Use font sizes between 12 and 14 points for body text. For headings, use a font size at least two points larger than the main text. Use fonts with serifs, as noted above. Use both upper and lowercase letters as you normally would, not all capitals, which reduces reading speed and comprehension. Use grammatically correct punctuation throughout.
When you want to emphasize a word or phrase, bold is your best option. Limit the use of italics and underlining. Use dark text on a light background. These are not complicated rules, but adhering to them consistently across your patient-facing materials makes a real difference in accessibility, particularly for older adults and individuals with low vision.
Patient Education Materials Assessment Tool (PEMAT)
One more tool I want to share with you before we close is the Patient Education Materials Assessment Tool (PEMAT), developed by the Agency for Healthcare Research and Quality (AHRQ). The PEMAT is a systematic method for evaluating and comparing the understandability and actionability of patient education materials. It is particularly useful for reviewing materials you are already using or developing new materials intended for diverse patient populations.
Understandability means that consumers of diverse backgrounds and varying levels of health literacy can process and explain the key messages. Actionability means that consumers can identify what they should do based on the information presented.
The PEMAT produces separate numeric scores for understandability and actionability by evaluating materials against a checklist of desirable characteristics.
Those characteristics include:
- The material's purpose is completely evident
- Does not include distracting content
- Uses common, everyday language; medical terms are defined when they must be used
- Uses the active voice
- Breaks information into short sections
- Uses visual cues such as arrows, boxes, bullets, bold text, and larger fonts to draw attention to key points
- Any visual aids support the main message
- Any numbers are clear and easy to understand
- Language and examples are familiar to the intended audience
- Images represent the audience's race, ethnicity, age, gender, and ability
- The material avoids perpetuating stereotypes.
Figure 9: PEMAT Annotated Example of Patient Education Material
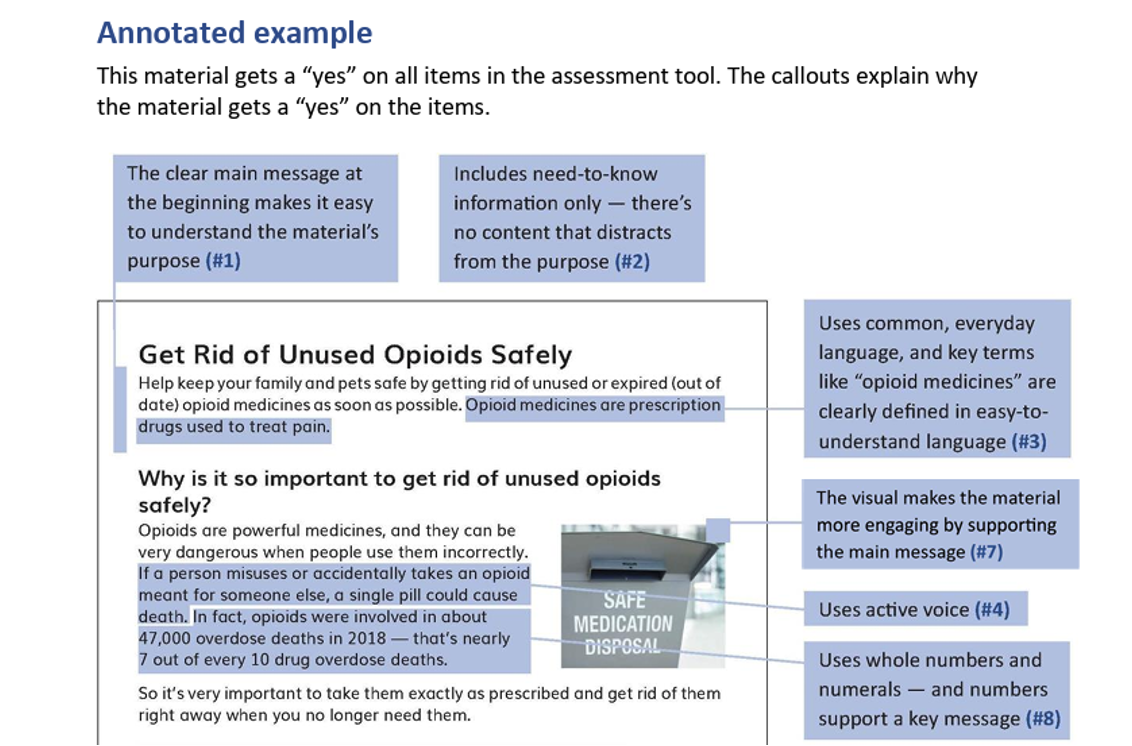
Figure 10: PEMAT Annotated Example of Patient Education Material (cont)
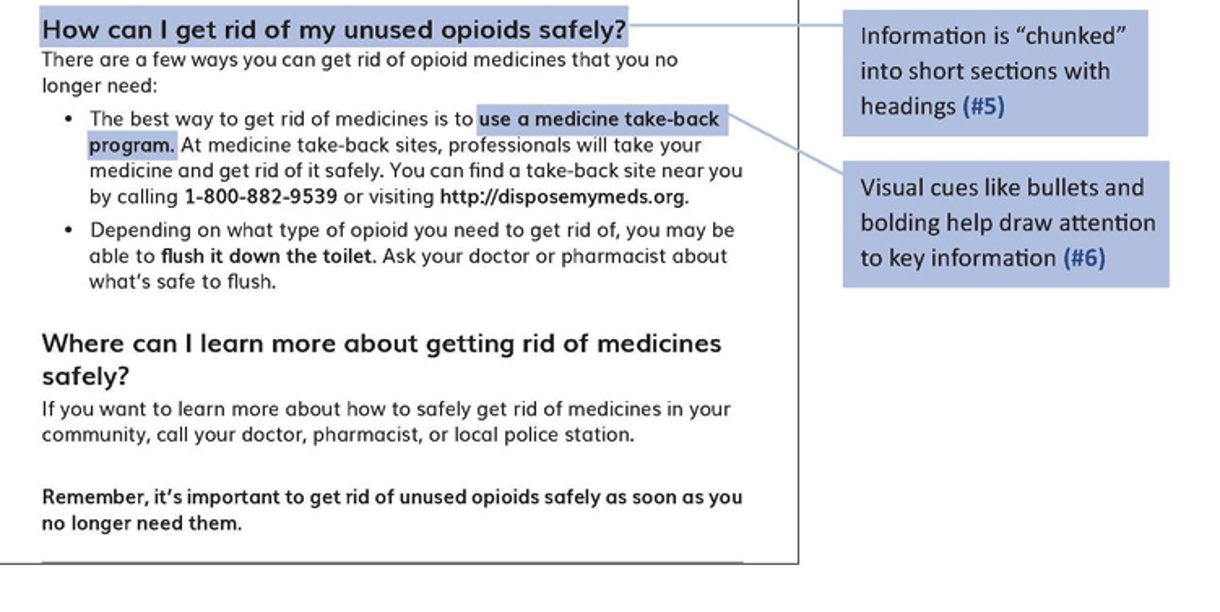
Image credit for Figures 9 and 10: National Library of Medicine
The PEMAT is easy to use and transforms the materials review process from a subjective exercise into a structured, reproducible evaluation. I encourage you to apply it to the next home program or handout you create.
Conclusion
Health literacy is not a specialized subspecialty within rehabilitation. It is the foundation of every therapeutic interaction we have. Every time we explain a diagnosis, provide a home program, demonstrate an exercise, or help a patient understand their discharge instructions, we are engaging in health communication. Whether that communication succeeds depends significantly on how well we have prepared to meet the patient where they are.
Let us briefly return to each of our learning outcomes to tie the threads together. We defined health literacy as the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions. We reviewed the key statistics and findings, including that only 12% of adults have proficient health literacy, that nearly 9 in 10 people in the U.S. have some degree of limited health literacy, and that the associated costs exceed $349 billion annually. We identified appropriate assessment tools, including the TOFHLA, REALM-SF, and Newest Vital Sign, as well as readability tools such as the Fry Readability Formula, the Flesch-Kincaid Grade Level Formula, and Microsoft Word's built-in statistics feature. And we explored the range of factors that influence health literacy, from individual characteristics to systemic barriers, and described practical techniques for facilitating health literacy in practice: plain language, Ask Me 3, teach-back, universal precautions, and culturally responsive communication.
Improved health literacy leads to improved outcomes. Patients who understand their condition and treatment are more likely to follow their exercise programs, adhere to recommendations, and achieve faster, more durable recovery. Better communication reduces emergency department use, hospital readmissions, and overall healthcare expenses. Enhanced patient engagement means individuals who sit with us at the goal-setting table, ask relevant questions, take charge of their healthcare situation, and become active participants in their own recovery. And addressing health literacy is one of the most direct paths we have toward reducing the health disparities that affect so many of the people we serve, including older adults, individuals with disabilities, and those from underserved populations.
You are already doing this work every day. My goal has been to give you language, tools, and strategies that make you even more effective at it. Thank you so much for being here.
References
Andrus, M. R., & Roth, M. T. (2002). Health literacy: A review. Pharmacotherapy, 22(3), 282–302.
Bader, M., Zheng, L., et al. (2022). Towards a more patient-centered clinical trial process: A systematic review of interventions incorporating health literacy best practices. Contemporary Clinical Trials, 116.
Muñoz, C., & Luckmann, J. (2005). Transcultural communication in nursing (2nd ed.). Delmar Learning.
Murugesu, L., Heijmans, M., Rademakers, J., & Fransen, M. P. (2022). Challenges and solutions in communication with patients with low health literacy: Perspectives of healthcare providers. PLoS ONE, 17(5), e0267782.
Parker, R. M., Baker, D. W., Williams, M. V., & Nurss, J. R. (1995). The test of functional health literacy in adults: A new instrument for measuring patients' literacy skills. Journal of General Internal Medicine, 10(10), 537–541.
Pfizer Inc. (2016). The newest vital sign: A health literacy assessment tool.
Razzaq, N., & Khan, E. F. (2023). Linguistics and physical therapy: A team approach to improving communication and rehabilitation outcomes. Pakistan Journal of Society, Education and Language (PJSEL), 9(2), 486–499.
van der Gaag, M., Heijmans, M., Spoiala, C., & Rademakers, J. (2022). The importance of health literacy for self-management: A scoping review of reviews. Chronic Illness, 18, 182234254.
Voigt-Barbarowicz, M., Dietz, G., et al. (2022). Patients' health literacy in rehabilitation: Comparison between the estimation of patients and health care professionals. International Journal of Environmental Research and Public Health, 19, 63522.
Weissberg, K. (2026, May). Health Literacy in Practice: Effective Communication and Education. PhysicalTherapy.com, Article 5024. Retrieved from: https://www.physicaltherapy.com
