Editor's note: This text-based course is a transcript of the webinar, GLP-1s and More: Pharmacology for Diabetes Mellitus and Other Endocrine Conditions, presented by Melissa Bednarek, PT, DPT, PhD, CCS.
*Please also use the handout with this text course to supplement the material.
Learning Outcomes
After this course, participants will be able to:
- Analyze the pathophysiology of diabetes mellitus, hypothyroidism, and osteoporosis with a focus on how medications may interrupt the process.
- Analyze the mechanism of action and side effects for each evidence-based medication class used in the treatment of diabetes mellitus, hypothyroidism, and osteoporosis.
- Analyze the implications for physical and occupational therapy for a patient taking a medication used in the treatment of diabetes mellitus, hypothyroidism, and osteoporosis.
Introduction
Thank you for joining me today. Before we get into the content, I want to share a few thoughts on pharmacology as a subject, because I have spent more than ten years teaching it, both to entry-level DPT students and to licensed therapists through continuing education. What I have found across both groups is that pharmacology tends to inspire a similar reaction: it feels overwhelming, and there is a quiet assumption that if you really need to know something, you can always look it up. I understand that impulse completely. The sheer number of medications, classes, and mechanisms can feel endless.
What I have also come to appreciate, though, is that licensed therapists increasingly recognize the value of having a deeper working knowledge of the medications their patients are taking. It is not about memorizing every drug on a formulary. It is about having sufficient understanding to make better clinical decisions, provide more meaningful patient education, and recognize when something does not quite add up in the examination room. That is what I hope to give you today.
My approach throughout this course will be consistent: I will start with the pathophysiology of a condition and then move on to how specific medications interrupt that pathophysiology. I have found this sequence makes pharmacology far less overwhelming because the medications stop feeling like a random list and start feeling like logical responses to a biological problem.
I should also note that this field is moving quickly. The second bullet in the standard continuing education disclosures, the one noting that new findings may change the validity of the information presented, is rarely more relevant than it is for GLP-1 receptor agonists. We are learning more about these medications almost weekly, and some of what I present today may already be evolving at the edges. With that context in place, let us get started.
Before we can discuss the pathophysiology of diabetes or the pharmacology used to manage it, I think it is helpful to introduce the cast of characters in glucose homeostasis. These are the biological actors whose normal functions set the stage for understanding both what goes wrong in diabetes and how our medications are trying to fix it.
Glucose and Insulin
The central character in this story is glucose. Along with fats and proteins, glucose is one of the body's primary fuel sources for generating adenosine triphosphate (ATP). ATP is the energy currency that powers virtually everything the body does, from cellular signaling to the contraction of skeletal muscle. For therapists, muscle contraction is the obvious clinical entry point: we need ATP to power the movements our patients are working so hard to regain and optimize.
ATP is stored only in very small amounts, which means the body must continuously regenerate it. Glucose plays a central role in that process. It can be broken down through glycolysis, a rapid process that does not require oxygen and that yields ATP quickly, though not in large quantities. This is why glycolysis is particularly important during short-duration, high-intensity activities where there simply is not enough time for the slower, oxygen-dependent process of cellular respiration. In cellular respiration, glucose, fats, and proteins are all metabolized to generate substantially more ATP, but this process requires oxygen and takes more time.
As a brief aside, this distinction maps neatly onto what we know about muscle fiber types. Type I, or slow-twitch, muscle fibers are equipped with the mitochondria and enzymatic machinery for cellular respiration. They are built for sustained effort. Type II, or fast-twitch, fibers rely more heavily on glycolysis for that rapid burst of energy production. This is a thread we could pull in many directions, but for our purposes today the important point is simply that glucose is the primary fuel source for the brain and for working muscle, and managing its availability is a high-stakes process.
One final point about glucose: excess glucose is not discarded. It is stored as glycogen, primarily in the liver and, to a lesser extent, in skeletal muscle. This stored glycogen can be converted back into glucose and released into the bloodstream when the body needs it. That dynamic will come back into focus when we discuss specific medication mechanisms.
If glucose is the star of our show, then insulin is the essential co-star. The relationship between insulin and diabetes is something that often confuses patients and, frankly, can trip up clinicians as well, so I want to take a moment to trace through the connection carefully.
Glucose is a large molecule. It cannot simply diffuse across the cell membrane into muscle or adipose tissue the way that small, lipid-soluble molecules can. It needs a transporter. Specifically, it depends on transporters called GLUT4, or glucose transporter type 4. In the resting state, between meals, these transporters do not sit on the cell surface. They are parked inside the cell in a vesicle, essentially waiting for a signal.
Insulin is that signal. When we eat a meal and blood glucose levels rise, the beta cells of the pancreas respond by releasing insulin into the bloodstream. Insulin travels to muscle cells and adipose tissue cells, where it binds to a specific receptor on the cell surface. That binding is what I think of as the key turning in the lock. When insulin binds its receptor, it triggers a cascade that moves the GLUT4 transporters from inside the cell up to the cell surface. With the transporters now available, glucose can enter the cell, blood glucose levels fall back toward normal, and the state of hyperglycemia is resolved (Navale & Paranjape, 2016).
This is the essential insulin story, and it is the story that breaks down in diabetes.
Figure 1: Pathophysiology of Type 2 DM, (Image: Licensed from Getty Images)
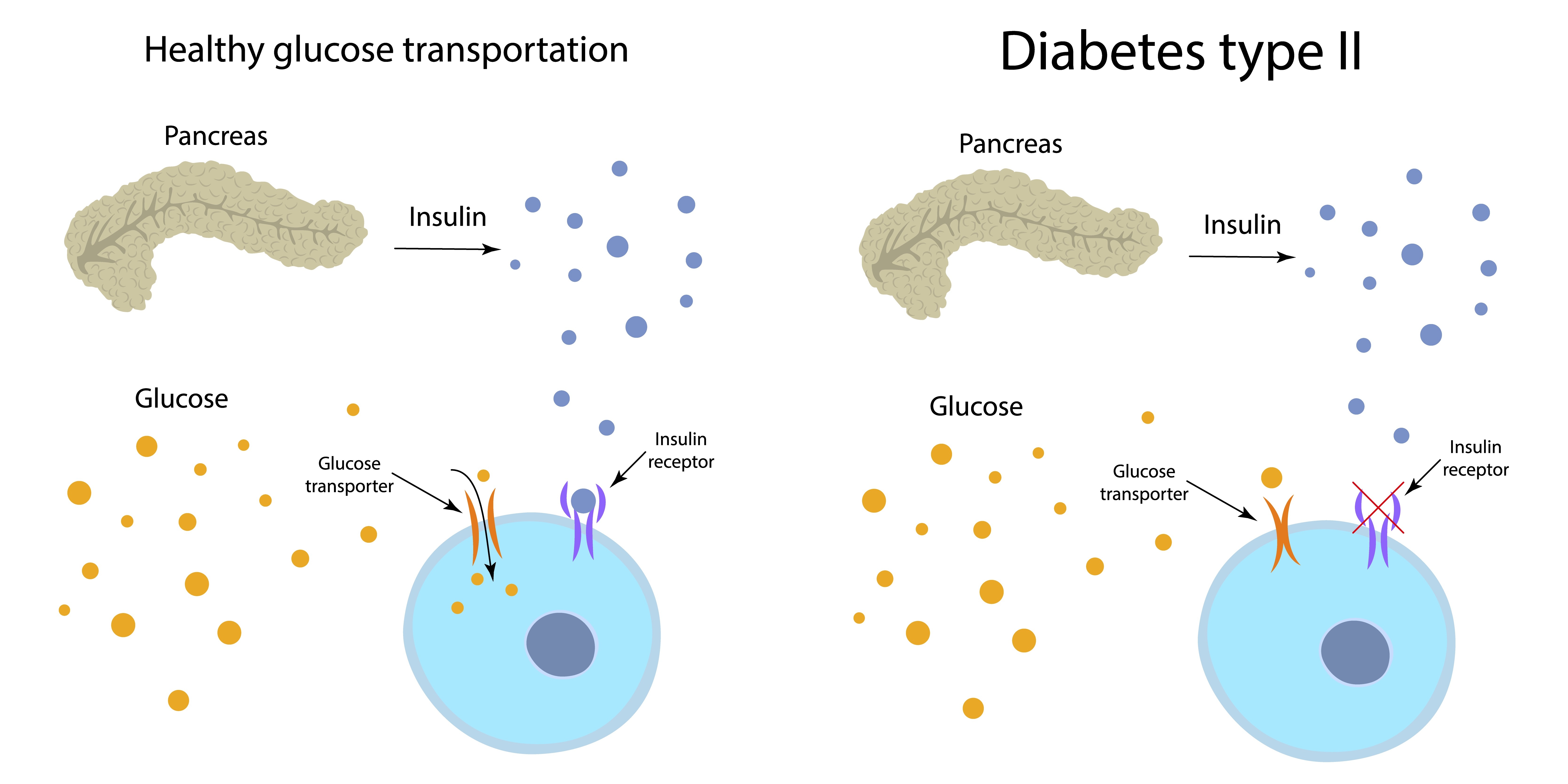
Understanding this mechanism makes the pathophysiology of both major types of diabetes much easier to follow. In type 1 diabetes, the body's own immune system attacks and destroys the beta cells of the pancreas. No beta cells means no insulin production, which means no signal to move the GLUT4 transporters. The key simply does not exist. In type 2 diabetes, insulin is produced, but the receptors on the muscle or adipose tissue cells do not respond to it. The key exists, but the lock will not turn. As we will see, this distinction drives very different treatment approaches (Ojo et al., 2023).
Pathophysiology of Type 2 DM
All forms of diabetes, including type 1, type 2, and gestational diabetes, share one defining feature: hyperglycemia, or chronically elevated blood glucose levels. That is the common thread. But the mechanism behind the hyperglycemia, and therefore the treatment approach, differs significantly.
Type 2 diabetes accounts for 90 to 95 percent of all diabetes diagnoses. Type 1 accounts for approximately 5-10 percent. This proportion matters clinically because the more common form, type 2, offers far more options for pharmacological and lifestyle management. It is worth noting that older terminology such as "adult-onset diabetes" for type 2 or "juvenile-onset diabetes" for type 1 is not only outdated but also increasingly inaccurate. Individuals who are younger and younger are being diagnosed with type 2 diabetes, and we will encounter all of this terminology in patient charts and medical records.
Gestational diabetes, first identified during pregnancy, involves an insulin resistance pattern more similar to type 2 than type 1. It deserves mention because it is not uncommon, and the patients we see in outpatient or home health settings may have a history of gestational diabetes that increases their lifetime risk of developing type 2.
Glucagon
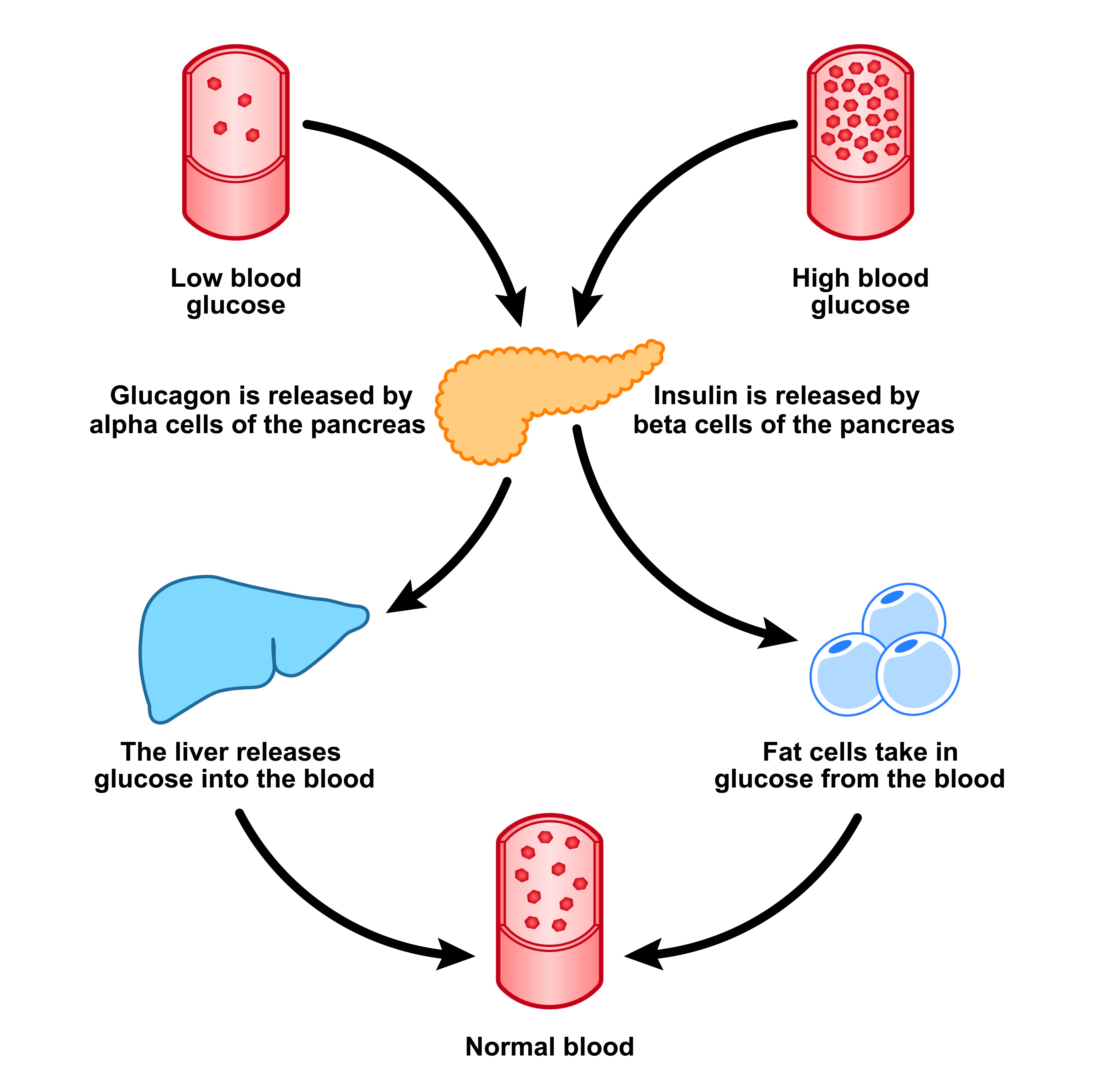
Glucagon is the functional counterpart to insulin, and understanding it is essential to appreciating the full system. While insulin facilitates the uptake of glucose into cells, glucagon does the opposite. It signals the liver to release stored glucose by converting glycogen back into glucose, raising blood glucose levels.
Glucagon is produced by the alpha cells of the pancreas, which sit adjacent to the beta cells that produce insulin. The trigger for glucagon release is not a meal but the absence of one. When blood glucose levels fall between meals, the alpha cells sense that drop and release glucagon. Glucagon then travels to the liver, instructs it to break down glycogen and release glucose into the bloodstream, and blood glucose levels return toward normal. So while insulin drives glucose out of the blood and into cells, glucagon pulls glucose back into the blood from liver stores. Together, they maintain the careful homeostatic balance that keeps blood glucose levels within a safe range.
This opposing relationship is not just a physiological curiosity. It has direct pharmacological implications. Several medication classes used in diabetes management work by modulating glucagon activity, and understanding glucagon's normal function helps make those mechanisms more intuitive.
Figure 2: Blood sugar regulation, (Image: Licensed from Getty Images)
GLP-1 and GIP
Now we come to the part of our cast that has attracted the most attention in recent years. Before I get into the specific medications, I want to introduce a term that is essential to understanding them: incretin.
Incretins are hormones naturally released by the gastrointestinal tract in response to a meal. Their primary function is to stimulate insulin secretion, but they do more than that, and the full scope of what they do is central to understanding why GLP-1 receptor agonists have become so significant in clinical practice.
There are two primary incretin hormones. The first is glucagon-like peptide-1, which is where GLP-1 takes its name. The second is glucose-dependent insulinotropic polypeptide, or GIP, which was formerly known as gastric inhibitory peptide. Both are released from the gut following a meal.
GLP-1 does several important things. It stimulates insulin release from the beta cells of the pancreas. It inhibits glucagon release from the alpha cells, which means it is working on both ends of the glucose regulation equation simultaneously. It slows gastric emptying, so food moves more slowly from the stomach into the small intestine. And it promotes a sense of satiety, or fullness. Those last two effects, slowed gastric emptying and increased satiety, are the mechanisms that connect GLP-1 to weight loss. When gastric emptying slows, the stomach feels full longer. When satiety is enhanced, the individual tends to eat less. These are not incidental side effects; they are direct physiological responses to GLP-1 activity (Holst, 2022).
GIP has some overlapping effects with GLP-1, including stimulating insulin release and slowing gastric emptying. It also supports bone health and promotes fat storage.
There is one more critical piece to know about both of these hormones: they are broken down by an enzyme called dipeptidyl peptidase-4, or DPP-4. This enzyme will come up again when we discuss the DPP-4 inhibitor medication class, so hold onto that fact.
SGLT-2
Our final character in the glucose homeostasis story is the sodium-glucose cotransporter 2, or SGLT2. This one takes us to the kidneys.
As part of their normal filtering function, the kidneys filter glucose out of the blood and mark it for excretion. However, in healthy individuals, most of that glucose is reabsorbed from the renal tubule back into the bloodstream before it is ever lost in the urine. The transporter that accomplishes this reabsorption is the SGLT2. It moves both sodium and glucose from the tubule back into circulation, which is why it is called a cotransporter.
This becomes relevant for diabetes because blocking the SGLT2, and therefore preventing that reabsorption, allows excess glucose to be excreted in the urine rather than returned to the bloodstream. That is precisely the mechanism targeted by one of our most important diabetes medication classes, the SGLT2 inhibitors, which we will discuss shortly.
With our cast of characters in place, glucose, insulin, glucagon, GLP-1, GIP, and SGLT2, we can now move into the pharmacological management of diabetes with much more context for why each medication class works the way it does.
Before we discuss medications, I want to briefly address why managing hyperglycemia is so critical. The nervous system is unique in that it can only use glucose as its energy source. It cannot run on fats or proteins the way muscle tissue can. This makes the nervous system particularly vulnerable to the toxic effects of chronically elevated blood glucose.
When blood glucose remains persistently high, as it does in poorly managed diabetes, it causes microvascular damage throughout the body. One of the most clinically significant consequences is peripheral neuropathy, a damage to the sensory nerve fibers in the extremities that manifests as numbness, tingling, pain, and loss of protective sensation. For physical and occupational therapists, peripheral neuropathy is not a background finding; it directly affects balance, gait, fall risk, functional mobility, and the safety of therapeutic exercise. Managing hyperglycemia is therefore not just the physician's job. It is something we have a direct professional stake in supporting.
Treatment for diabetes is monitored through two primary mechanisms: real-time blood glucose checks and longer-term blood work measuring hemoglobin A1C, or HbA1C.
Hemoglobin A1C reflects average blood glucose levels over approximately the past two to three months. The reason for this time frame is tied to the biology of red blood cells: the lifespan of a red blood cell is roughly 120 days, or about four months. What the A1C measures is the proportion of hemoglobin on red blood cells that has been glycated, meaning glucose has bound to it. The more time spent in a state of hyperglycemia, the more glycated hemoglobin accumulates. Because we are essentially measuring a historical record embedded in living cells, there is no value in testing A1C more frequently than every three to four months. For patients meeting treatment goals, twice-yearly testing may be sufficient. For those whose management is still being optimized, testing up to four times per year is appropriate.
For most patients, a treatment goal of A1C at or below 7 percent is considered reasonable. For older adults or those with significant comorbidities, a slightly higher target of below 8 percent may be appropriate, as aggressive glucose lowering in these populations can increase the risk of hypoglycemia, which carries its own serious consequences.
This balance between too high and too low is one of the central themes I will return to throughout this course. Pharmacological management of diabetes is fundamentally an exercise in finding and maintaining that balance.
Pharmacologic Management
Because the only treatment available for type 1 diabetes is insulin, that is where the treatment options narrow significantly. For type 2 diabetes, however, there are multiple medication classes with different mechanisms of action, and patients are commonly on more than one simultaneously (American Diabetes Association, 2026). Before I explain why polypharmacy is common in diabetes management, let me work through each class.
More commonly used medications in the treatment of Type 2 DM include:
- Biguanide
- Dipeptidyl peptidase 4 (DPP-4) inhibitors
- Glucagon-like peptide 1 (GLP-1) receptor agonists
- Dual glucose-dependent insulinotropic polypeptide (GIP) and GLP-1 receptor agonists
- Sodium-glucose cotransporter 2 (SGLT2) inhibitors
- Sulfonylureas
- Thiazolidinediones (TZDs)
Biguanide
The first and most foundational medication in type 2 diabetes management is metformin, the only drug in the biguanide class. The brand name is Glucophage, though you will most often encounter it by its generic name. Metformin is administered orally and has been available for decades. It is typically the first-line agent prescribed when a patient is newly diagnosed with type 2 diabetes.
Metformin works primarily at the liver. Remember that the liver stores glucose as glycogen and can release that stored glucose back into the bloodstream. In a person with type 2 diabetes, the liver may release excess glucose even when blood glucose levels are already elevated, compounding the hyperglycemia. Metformin suppresses this hepatic glucose production, telling the liver to hold back the release of stored glucose and thereby reducing blood glucose levels.
What makes metformin particularly well-suited to first-line use is its side effect profile. The most notable side effect is gastrointestinal, primarily diarrhea, which can often be minimized by taking the medication with food. Critically, two common concerns with other diabetes medications, hypoglycemia and weight gain, are not associated with metformin. This makes it a more favorable option from a safety standpoint, particularly for patients who are newly diagnosed and whose medication regimen is still being established.
Dipeptidyl Peptidase 4 Inhibitors
The next class builds directly on our earlier discussion of incretin hormones. If GLP-1 and GIP have beneficial effects on blood glucose regulation, and if they are broken down by the enzyme DPP-4, then one logical pharmacological strategy is to inhibit DPP-4. That is exactly what this medication class does.
DPP-4 inhibitors
- Sitagliptin (Januvia)
- Saxagliptin (Onglyza)
- Linagliptin (Tradjenta)
- Alogliptin (Nesina)
Dipeptidyl peptidase-4 inhibitors, or DPP-4 inhibitors, are administered orally and work by preventing the breakdown of GLP-1 and GIP, allowing these naturally occurring incretins to remain active in the body longer and exert their glucose-lowering effects more fully. You will often hear this class referred to as the "gliptins," because most of the generics carry that suffix: sitagliptin (Januvia), saxagliptin (Onglyza), linagliptin (Tradjenta), and alogliptin (Nesina).
DPP-4 inhibitors facilitate insulin secretion after meals, slow gastric emptying, and generally do not carry a significant risk of hypoglycemia. Side effects can include gastrointestinal symptoms such as nausea and diarrhea, as well as less intuitive symptoms such as headache, nasal congestion, sore throat, and joint pain.
Glucagon-Like Peptide 1 Agonist
The GLP-1 receptor agonist class is most likely the one most responsible for drawing many clinicians to this course. These medications are what I call incretin mimetics: they mimic the function of naturally occurring GLP-1, binding to the same receptors and producing the same effects. However, they offer a critical advantage over the body's own GLP-1: they are resistant to DPP-4-mediated breakdown. This means they remain active longer and can sustain their effects, unlike endogenous GLP-1 (Cleveland Clinic, 2026; Drucker, 2024).
GLP-1 agonist
- Dulaglutide (Trulicity)
- Exenatide (Byetta)
- Exenatide extended-release (Bydureon)
- Liraglutide (Victoza)
- Lixisenatide (Adlyxin)
- Injectable semaglutide (Ozempic)
- Oral semaglutide (Rybelsus)
The GLP-1 receptor agonists are, with one exception, administered by injection. The exception is oral semaglutide, marketed as Rybelsus. The injectable forms include liraglutide, exenatide, dulaglutide, albiglutide, and injectable semaglutide, among others. Current evidence generally suggests that the injectable forms are more effective than the oral form.
What this class does: it stimulates insulin secretion in a glucose-dependent manner, inhibits glucagon release, slows gastric emptying, and promotes satiety. The clinical effects of these medications go beyond glycemic control, and that is what I want to address directly.
We cannot discuss GLP-1 receptor agonists without discussing weight loss, because that is the context in which most of your patients, and frankly most of the popular press, know these medications. Here is the clearest way I can frame the relationship between diabetes and weight-loss medications: in many cases, they are the same drug with different brand names and different FDA-approved indications.
Take liraglutide, for example. Under the brand name Victoza, it is FDA-approved for the treatment of type 2 diabetes. Under the brand name Saxenda, the same molecule is FDA-approved for weight loss in adults and children ages 12 and older. The generic, the compound, and the mechanism of action are identical. What differs is the approved indication.
The same pattern applies to semaglutide. Injectable semaglutide, marketed as Ozempic, is approved for the management of type 2 diabetes. The same molecule marketed as Wegovy is approved for weight loss in adults and children ages 12 and older. Oral semaglutide, sold as Rybelsus, is approved for the treatment of type 2 diabetes.
The most commonly discussed side effects of GLP-1 receptor agonists are nausea and vomiting, which are especially prominent when starting the medication or when the dose is increased. This is worth knowing as a clinician because a patient adjusting to a new or increased dose of a GLP-1 may experience reduced appetite and energy, which could affect their participation in therapy.
One question that frequently arises and is highly relevant to our practice is the effect of GLP-1 receptor agonists on muscle mass. The literature focused on diabetes does not address this extensively, but it is a well-known clinical concern among patients using these medications for weight loss. Anecdotally and from early body composition data, maintaining adequate protein intake and incorporating resistance training appear to be meaningful strategies for minimizing muscle loss in patients using these medications. That is an area where we as therapists can provide real value.
Dual GIP and GLP-1 Receptor Agonists
A newer class extends the incretin mimetic concept by targeting both GLP-1 and GIP receptors simultaneously. Currently, there is one medication in this class: tirzepatide. Under the brand name Mounjaro, tirzepatide is approved for the treatment of type 2 diabetes. Under the brand name Zepbound, the same molecule is approved for weight loss in adults.
The mechanism combines the GLP-1 effects I already described with the additional insulin-stimulating and gastric-slowing effects of GIP. Side effects are similar to those of the GLP-1 receptor agonists: nausea and vomiting, particularly when initiating treatment or increasing the dose.
The FDA has approved three medications specifically for weight loss as of my preparation of this content: liraglutide (Saxenda), semaglutide (Wegovy), and tirzepatide (Zepbound) (National Institute of Diabetes and Digestive and Kidney Diseases, 2026b). It is important to hold this information loosely, as the space is evolving rapidly and additional approvals are likely to follow.
Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors
Returning to our cast of characters, recall that the sodium-glucose cotransporter 2 in the kidney is responsible for reabsorbing glucose from the renal tubule back into the bloodstream. SGLT2 inhibitors work by blocking this transporter, allowing excess glucose to be excreted in the urine rather than being recirculated. The result is a reduction in blood glucose levels through a mechanism that is entirely separate from insulin.
You can identify drugs in this class by their shared suffix, gliflozin:
SGLT2 inhibitors:
- Bexagliflozin (Brenzavvy)
- Canagliflozin (Invokana)
- Dapagliflozin (Farxiga)
- Empagliflozin (Jardiance)
One side effect that follows logically from the mechanism is an increased risk for genital yeast infections. Yeast uses glucose as a food source, and when more glucose is present in the urine, yeast infections become more likely. Patients should be informed about this risk.
It is also worth knowing that SGLT2 inhibitors have demonstrated clinical benefits beyond glycemic control. They have been studied in heart failure and kidney disease, and empagliflozin in particular is one of what cardiologists now call the "Fantastic Four" drug classes in the treatment of heart failure with reduced ejection fraction. If you see SGLT2 inhibitors on the medication lists of patients you are treating for cardiac conditions, this broader context helps explain their presence.
Sulfonylureas
The sulfonylureas are among the oldest classes of diabetes medications, available since the 1950s. Examples include glimepiride (Amaryl), glipizide (Glucotrol), and glyburide (Diabeta, Micronase). These drugs work by stimulating the beta cells of the pancreas to produce and release more insulin, essentially pushing the pancreas to produce as much insulin as possible.
The major clinical concerns with sulfonylureas are hypoglycemia and weight gain. Because these medications increase insulin levels regardless of blood glucose levels, the risk of hypoglycemia is real and significant. For therapists, this is particularly relevant during exercise sessions, as exercise has its own glucose-lowering effects that can combine with the drug's effect to produce hypoglycemia. Weight gain is a common side effect because increased insulin availability promotes the uptake and storage of nutrients.
Sulfonylureas remain in use because they are effective and affordable, but they are generally not preferred first-line agents due to their side-effect profile.
Thiazolidinediones
The thiazolidinediones, universally abbreviated as TZDs because their full names are difficult to pronounce, include rosiglitazone (Avandia) and pioglitazone (Actos). Rather than stimulating insulin production, as sulfonylureas do, TZDs act peripherally. They act on muscle and adipose tissue to improve cells' responsiveness to insulin, making it easier for insulin to unlock GLUT4 transporters and facilitate glucose uptake.
TZDs also reduce hepatic glucose production to some degree. Because they work by making existing insulin more effective rather than increasing insulin levels directly, hypoglycemia is less of a concern than with sulfonylureas. However, TZDs carry concerns about heart failure risk and lower extremity edema, which are important considerations for therapists working with this patient population. Any patient on a TZD who presents with new or worsening lower extremity swelling warrants attention and, if unexplained by musculoskeletal causes, communication with the referring provider.
Less Common Medications
Beyond the major classes, several additional medications used to treat type 2 diabetes are less commonly prescribed but worth knowing.
Alpha-Glucosidase Inhibitors
Examples include acarbose (Precose) and miglitol (Glyset). Alpha-glucosidase is an enzyme in the digestive system that facilitates the breakdown of dietary starches into simple sugars for intestinal absorption. By inhibiting alpha-glucosidase, alpha-glucosidase inhibitors slow the absorption of glucose from the gut, blunting the post-meal rise in blood glucose. The main side effects are gastrointestinal, specifically flatulence and diarrhea, resulting from undigested starches reaching the large intestine.
Bile Acid Sequestrants
The bile acid sequestrant used in the treatment of diabetes is colesevelam (Welchol). This is perhaps the most surprising entry in this list. Bile acid sequestrants are primarily used as cholesterol-lowering medications. The medication binds bile acids in the digestive tract; when the body has less available bile acid, it turns to LDL cholesterol as a replacement, effectively pulling LDL out of circulation and lowering it. Their clinical application in diabetes is recognized, but the mechanism by which they lower blood glucose is not fully understood. I will be straightforward: I do not have a clear mechanistic explanation to offer here. The connection exists and is clinically documented, but it is one of the less illuminated corners of diabetes pharmacology. Side effects include flatulence and constipation.
Dopamine-2 Agonists
Bromocriptine (Cycloset) is the example here. Bromocriptine is more recognizable to many clinicians as a treatment used in Parkinson's disease, where its dopaminergic effects are the point. Its application in diabetes operates through a different pathway: it is thought to reset circadian rhythms in the hypothalamus, which regulate, among other things, daily blood glucose patterns (Shivaprasad & Kalra, 2011). Nausea is the primary side effect.
Meglitinides
Examples include nateglinide (Starlix) and repaglinide (Prandin). This class shares some functional similarities with sulfonylureas, as meglitinides stimulate insulin release from pancreatic beta cells. However, their release mechanism is more closely tied to ambient glucose levels, making their action more calibrated to actual need. Hypoglycemia and weight gain are still potential side effects, but these concerns are generally less pronounced with meglitinides than with sulfonylureas.
Multiple Medication Question
Before moving to insulin, I want to address a question that deserves explicit attention: why are patients so often on multiple medications for the same condition? The answer lies in the diversity of mechanisms I have just described. Each medication class addresses hyperglycemia through a different physiological pathway. Metformin reduces hepatic glucose release. SGLT2 inhibitors increase urinary glucose excretion. GLP-1 agonists mimic incretin effects. Sulfonylureas squeeze the pancreas for more insulin. TZDs improve peripheral insulin sensitivity.
By combining agents with different mechanisms, prescribers can address the same problem from multiple angles simultaneously and keep the dose of each agent lower. Lower doses generally mean fewer and milder side effects. This is a universal principle in pharmacology: combination therapy with lower individual doses often produces better outcomes with fewer adverse effects than high-dose monotherapy. When you see a patient on metformin plus a GLP-1 plus an SGLT2 inhibitor, that combination reflects a deliberate strategy, not redundancy.
Insulin
Insulin is the cornerstone of type 1 diabetes management and is often incorporated into type 2 management as the disease progresses. What I want to do here is give you a clear framework for understanding the different types of insulin and why those distinctions matter for clinical practice.
First, a critical pharmacokinetic point: insulin cannot be taken orally. If swallowed, it would be broken down by digestive enzymes in the stomach and small intestine and would never reach circulation. This is why insulin is always administered directly into the body, either intravenously, through an insulin pump, or by subcutaneous injection (American Diabetes Association, n.d.; McCulloch, 2018b).
The subcutaneous route is the most common for self-administered insulin, and the specifics of subcutaneous injection are clinically important. Subcutaneous tissue, the layer of adipose tissue just beneath the skin, has a lower blood supply than muscle tissue. This matters because the rate of absorption from the injection site into the bloodstream is intentionally slowed by the low vascularity. If insulin were injected directly into muscle, which has robust blood supply, it would be absorbed much more rapidly, producing a sudden spike in circulating insulin that could cause dangerous hypoglycemia. The slower, more controlled release from subcutaneous tissue is by design.
Patients who self-inject insulin rotate their injection sites to prevent inflammation and lipodystrophy at any single site. Common sites include the abdomen, the thighs, and the upper arms. As we will discuss in the therapy implications section, the site of a recent injection matters for how we structure an exercise session.
All insulins differ along three key parameters: onset of action (how quickly they start working), peak action (when their effect is maximal), and duration of action (how long they remain effective). There are four categories.
Insulin: Ultra-Rapid Acting
This type is designed to dissolve rapidly at the injection site and begin lowering blood glucose almost immediately before a meal. The onset is 5 to 15 minutes, peak action occurs at 45 to 75 minutes, and duration is 2 to 4 hours. Examples include lispro (Humalog), aspart (Novolog), and glulisine (Apidra). In acute care settings, ultra-rapid-acting insulin is the type used in sliding-scale protocols: blood glucose is checked just before a meal, and a dose is calibrated to the current glucose level. Increasing the number of units of ultra-rapid-acting insulin will lower blood glucose more, but it will not extend the duration of effect.
Insulin: Rapid-Acting
Also called regular insulin, this type has a 30-minute onset, peaks at 2 to 4 hours, and lasts 5 to 8 hours. Examples include Humulin R and Novolin R. It takes longer to get going and lasts longer than ultra-rapid-acting insulin.
Insulin: Intermediate Acting
Also called NPH insulin, where NPH stands for neutral protamine hagedorn, this type has an onset of approximately 2 hours, peaks at 4 to 12 hours, and has a duration of 8 to 18 hours or longer. It is slower-acting and longer-lasting than regular insulin, designed to provide coverage over a larger portion of the day. Examples include Humulin N and Novolin N
Insulin: Long-Acting
This type has an onset of about 2 hours, does not produce a pronounced peak, and provides a steady, basal insulin level for approximately 20 to 24 hours. The most common example is insulin glargine (Lantus). Long-acting insulin is typically taken once daily and serves as a baseline to maintain stable blood glucose levels around the clock, with mealtime coverage provided by a faster-acting insulin as needed.
A patient may be on more than one type of insulin at the same time. For example, they might take a long-acting insulin daily as their basal dose and add an ultra-rapid-acting insulin before meals. Understanding which type of medication a patient has recently taken, when they took it, and where they injected it becomes directly relevant to how we structure therapy sessions.
Insulin: Adverse Effects
Whenever we are managing a patient whose medication regimen could cause hypoglycemia, including insulin, sulfonylureas, and meglitinides, we need to be prepared to recognize and respond to a hypoglycemic episode. Hypoglycemia is defined as blood glucose below 70 mg/dL.
The clinical presentation of hypoglycemia spans two physiological categories. Sympathetic nervous system activation produces tachycardia, elevated blood pressure, palpitations, diaphoresis (sweating), tremors, and irritability. Parasympathetic symptoms may include nausea and intense hunger. As hypoglycemia progresses, central nervous system effects emerge: headache, dizziness, mental dullness, confusion, and even amnesia. In severe cases, seizures, paralysis, paresthesia, visual changes, and loss of consciousness can occur.
Case Example
I want to share an experience that brought this home for me clinically. I was covering a pulmonary rehabilitation clinic on a per-diem basis, which meant I had no long-standing history with the patients in the program. A gentleman approached me near the end of his session, about 11:30 in the morning, and told me he needed to leave immediately. He needed to go meet a friend for lunch. He was irritable, restless, and clearly agitated. None of that was immediately alarming on its own. It was 11:30, he was hungry, and he had a social commitment. That all made complete sense.
But as I spoke with him, I noticed something that did not fit: beads of sweat were running down his forehead. He was participating in aerobic exercise, and we always want to challenge our pulmonary patients appropriately, but this level of diaphoresis seemed out of proportion to the activity. Something about it struck me. I asked if he was diabetic. He said yes. I asked if there was any chance his blood sugar might be low. He denied it firmly and had a ready explanation for every symptom I was silently cataloging.
Eventually, I persuaded him to take a glucose tablet. Within five minutes, he was a completely different individual. The irritability and urgency were gone, and his affect normalized. That experience has stayed with me because the signs were individually explainable, except for the sweating. It was the one symptom that did not fully fit the narrative he was offering.
Hypoglycemia unawareness
One additional clinical nuance worth knowing: patients who experience frequent episodes of hypoglycemia can develop what is called hypoglycemia unawareness. Their autonomic nervous system response becomes blunted, and they may not experience the early warning signs of a dropping blood glucose until the level is dangerously low. These patients require especially careful monitoring.
Continuous glucose monitors, or CGMs, such as the Dexcom and the Freestyle Libre, are valuable tools for managing this risk. They provide real-time blood glucose readings through a small sensor worn on the skin, typically on the arm or abdomen, linked to a smartphone application. For therapists who may not be permitted to perform fingerstick glucose checks under their state practice act, a patient with a CGM can self-report their real-time glucose reading, which can meaningfully inform clinical decision-making.
The clinical rule is simple: if a patient may be hypoglycemic, provide glucose. Even if the presentation is ambiguous and you are not certain, providing a modest glucose source will not cause meaningful harm if blood glucose turns out to be normal. However, it can be life-saving if the patient is hypoglycemic.
The amounts of glucose needed to bring a patient out of a hypoglycemic episode are often surprisingly small. Four ounces of orange juice, six ounces of regular soda (not diet), three graham crackers, six jelly beans, or three to four glucose tablets are all sufficient. Keep glucose tablets available in your clinical space as a matter of routine. After providing glucose, monitor the patient and allow time for the blood glucose to stabilize before resuming activity.
Therapy Implications
Understanding the pharmacology of diabetes medications is not an academic exercise for us as therapists. It has direct, practical implications for how we plan and deliver treatment.
First Implication
The first implication is the most fundamental: any patient taking insulin, a sulfonylurea, or a meglitinide is at risk for hypoglycemia, and we must monitor for it actively throughout our sessions. The signs and symptoms I described earlier, including the sympathetic manifestations of sweating, tremor, and irritability, are the ones we can observe directly. When we see them in a patient we know to have diabetes and to be on one of these medications, hypoglycemia belongs high on the differential.
Second Implication
The second implication involves the relationship between insulin injection sites and exercise-induced blood flow. Because subcutaneous insulin is absorbed slowly due to the relatively low vascularity of that tissue layer, anything that increases blood flow to an injection site will accelerate insulin absorption. Exercise is one of the most potent stimuli for increasing regional blood flow.
If a patient has recently administered a mealtime dose of rapid- or ultra-rapid-acting insulin into their thigh, and we then have them perform lower extremity exercise, we are increasing blood flow to that injection site. This can cause the insulin to be absorbed more quickly than intended, raising the risk of hypoglycemia. The patient's dosing was calibrated based on an expected absorption rate in the absence of exercise. Our intervention changed that.
This is why it is worth asking patients with diabetes about their most recent insulin injection: when, which type, and where. It takes seconds, and it can meaningfully change how you sequence your session.
Third Implication
The third implication concerns one of the most clinically elegant mechanisms in exercise physiology, one I did not fully appreciate for years. Understanding it has genuinely changed how I think about exercise prescription for patients with diabetes.
Here is the mechanism: insulin is not the only way to move GLUT4 transporters to the cell surface. Muscle contraction itself does it independently of insulin.
When large muscle groups contract rhythmically during aerobic exercise, walking, cycling, or swimming, the mechanical stimulus of contraction triggers those same GLUT4 transporters to migrate from inside the cell to the cell surface. Glucose can then enter the cell through facilitated diffusion, completely independent of insulin. There is no insulin required. The muscular work alone is sufficient.
This is an insulin-independent glucose uptake pathway. It explains why regular aerobic exercise can reduce insulin requirements in patients with type 2 diabetes. By consistently engaging in moderate-intensity aerobic activity, patients can reduce or, in some cases, eliminate their need for insulin. The contracting muscles are providing the signal that insulin would otherwise have to provide (Colberg et al., 2010; McCulloch, 2018a).
These effects persist for 24 to 72 hours following a single bout of moderate-intensity aerobic exercise (Colberg et al., 2016; Messina et al., 2023). This has important clinical implications. A patient who exercises with you on Tuesday may remain at elevated risk for hypoglycemia on Wednesday and even Thursday, depending on their insulin regimen. If their insulin dose has not been adjusted to account for the ongoing insulin-sensitizing effect, they may experience hypoglycemia well after the exercise session ends. Educating patients to monitor blood glucose for a longer period after exercise is a meaningful intervention.
The preponderance of the exercise and diabetes literature focuses on aerobic activity, and the insulin-independent GLUT4 pathway I just described is most well-characterized in the context of rhythmic, large-muscle-group aerobic exercise. However, there is growing evidence supporting the addition of resistance training.
Research in obese postmenopausal women with type 2 diabetes has demonstrated that adding resistance training to an aerobic exercise program produces meaningful improvements in insulin sensitivity beyond those achieved with aerobic training alone (Cuff et al., 2003). Insulin sensitivity, the degree to which cells respond to insulin and allow glucose uptake, is at the heart of the pathophysiology of type 2 diabetes. Any intervention that improves it is directly therapeutic.
The American College of Sports Medicine recommends a target of more than 150 minutes per week of moderate-intensity aerobic exercise for patients with diabetes to achieve significant reductions in HbA1C. Greater exercise volume results in greater reductions in A1C than lower-volume programs (Umpierre et al., 2011). This is a parameter we can actively influence in clinical practice.
Given these mechanisms, pre-exercise blood glucose levels provide critical information for clinical decision-making in patients with diabetes. If a patient's blood glucose level is below 100 mg/dL before beginning aerobic exercise, they should probably have a small snack before starting. With the insulin-independent uptake pathway activated during exercise, we are about to lower their blood glucose further through a mechanism that bypasses their insulin regimen. Starting from a lower baseline increases the risk of hypoglycemia during or after the session.
Conversely, if a patient's blood glucose is greater than 250 mg/dL prior to exercise, exercise should be approached with caution. At this level, the individual is not metabolically stable, and while exercise would ultimately lower blood glucose, proceeding when glucose is dangerously elevated is not appropriate. If blood glucose exceeds 300 mg/dL, exercise is not appropriate until the patient is more stable and their regimen is better controlled.
Hypothyroidism
The second endocrine condition we will address today is hypothyroidism, which is significantly more common in physical and occupational therapy patient populations than its prominence in our training might suggest. Many patients we see for musculoskeletal, neurological, or cardiopulmonary conditions will have hypothyroidism on their problem list or levothyroxine on their medication list. Understanding what this means for the whole patient is part of practicing at the full scope of our profession.
The thyroid gland is a small, butterfly-shaped gland located in the front of the neck. Its primary products are two thyroid hormones: thyroxine (T4) and triiodothyronine (T3). These hormones regulate metabolic rate, among many other functions. When the thyroid is underactive, as in hypothyroidism, T3 and T4 are undersecreted, leading to a reduced metabolic rate and wide-ranging physiological consequences (Davis & Phillippi, 2022; Mayo Clinic, 2026; National Institute of Diabetes and Digestive and Kidney Diseases, 2026a).
To understand how thyroid dysfunction is classified, it is useful to distinguish between primary and secondary endocrine pathology. A primary endocrine disorder involves a problem with the gland itself, in this case, the thyroid gland, which does not produce sufficient hormone. A secondary endocrine disorder involves a problem with the regulatory signal coming from outside the gland, in this case, the pituitary gland or the hypothalamus, failing to properly stimulate the thyroid to produce its hormones.
The causes of primary hypothyroidism include genetic factors, autoimmune conditions, radiation therapy (which can damage thyroid tissue), surgical removal of the thyroid gland, and certain medications. Among autoimmune causes, Hashimoto's thyroiditis is the most common cause of primary hypothyroidism. It is worth noting the autoimmune thread connecting our three conditions today: type 1 diabetes involves autoimmune destruction of pancreatic beta cells, and Hashimoto's thyroiditis involves autoimmune attack on the thyroid. Celiac disease is another autoimmune condition associated with hypothyroidism.
Surgical removal of the thyroid is sometimes performed to treat conditions such as hyperthyroidism, thyroid cancer, or a goiter producing excess hormone. When the thyroid gland is removed, the result is a state of hypothyroidism, and the patient will require lifelong thyroid hormone replacement therapy.
The clinical presentation of hypothyroidism reflects the consequences of a slowed metabolic rate: fatigue, weight gain, cold intolerance, constipation, dry skin, bradycardia, and, in some patients, depression. A specific and diagnostically notable feature of hypothyroidism is myxedema, the accumulation of fatty, mucous deposits, particularly under the eyes, in the hands, and in the feet. Myxedema can also produce swelling in the throat, leading to hoarseness and slurred speech. These are symptoms specific enough to hypothyroidism that their presence should prompt consideration of the diagnosis.
Hypothyroidism is diagnosed through laboratory measurement of T4 and thyroid-stimulating hormone, or TSH. TSH is produced by the anterior pituitary and serves as the upstream signal instructing the thyroid to produce T3 and T4. In primary hypothyroidism, T4 levels will be low, and TSH will typically be elevated, as the pituitary attempts to compensate for the underactive thyroid by sending stronger signals. Monitoring both TSH and T4 together gives a more complete picture of thyroid function and treatment response.
Levothyroxine
The treatment for hypothyroidism is, in most cases, a single medication: levothyroxine, most commonly known by the brand name Synthroid, though Levo-T and other formulations exist. Levothyroxine is a synthetic form of T4, administered orally on a daily basis. It is the most prescribed medication in the United States.
Monitoring treatment effectiveness is done through periodic TSH testing. Early in treatment, TSH may be checked every four weeks until stable levels are achieved. Once the patient is stabilized on a dose, monitoring intervals typically extend to every 12 weeks, then to every 6 months.
The primary side effect concern with levothyroxine is iatrogenic hyperthyroidism, which occurs when the dose is too high or the patient has been on an excessive dose for too long. Hyperthyroidism presents with symptoms that are essentially the mirror image of hypothyroidism: elevated metabolic rate, tachycardia, weight loss, heat intolerance, and increased anxiety. A persistently elevated T4 level due to excessive levothyroxine dosing also carries a risk to bone health, a connection that directly bridges to our next topic: osteoporosis.
Therapy Implications
One of the most practically important messages I want to convey about hypothyroidism is the possibility of encountering an undiagnosed endocrine disorder masquerading as a musculoskeletal complaint. Hypothyroidism can cause muscle aches, tenderness, stiffness, joint pain, and swelling of the small joints of the hands and feet, symptoms that can mimic arthritis, tendinopathy, or chronic pain of undetermined origin. If you are seeing a patient whose musculoskeletal presentation does not quite match a plausible mechanism of injury or evolves in unexpected ways, it is worth keeping an endocrine disorder on your clinical radar.
Carpal tunnel syndrome is another symptom associated with hypothyroidism that can present to therapy. If a patient presents with carpal tunnel symptoms without a clear mechanical explanation, and particularly if they also describe other diffuse symptoms like fatigue, weight gain, or cold intolerance, hypothyroidism is worth flagging with the referring provider.
For patients who have been diagnosed with hypothyroidism and have been started on levothyroxine, our role shifts. We should monitor for signs that the medication is producing hyperthyroidism. Tachycardia, unexplained weight loss, tremor, excessive diaphoresis, or a significantly elevated resting heart rate during or after exercise should be noted and communicated to the medical team, as they may indicate a need to adjust the dose.
Therapists can also play a meaningful role in helping patients recover their functional capacity as their metabolic rate normalizes with treatment. A patient who has been living with unmanaged hypothyroidism may have significantly reduced aerobic capacity and activity tolerance. Once the medication is on board and their metabolic rate begins to increase, a carefully graded aerobic training program can help them rebuild the activity tolerance that their condition has diminished.
Osteoporosis
The third condition we will address is osteoporosis. To understand the pharmacology, we first need to correct a common misconception: bone is not a static tissue. I held onto that mental model longer than I should have as a student, and it made everything about bone metabolism harder to understand than it needed to be. Bone is extraordinarily dynamic. It is constantly being formed and resorbed, with those two processes in continuous balance.
Three cell types are central to bone physiology. Osteoclasts are the bone-resorbing cells. They break down existing bone matrix and release the minerals stored within it. Osteoblasts are the bone-forming cells. They synthesize new bone matrix and mineralize it. Osteocytes are former osteoblasts that have become embedded within the bone matrix, where they serve as mechanosensors and communicate information about mechanical loading back to the remodeling system.
In healthy bone, osteoclast and osteoblast activity are balanced. The rate at which bone is broken down is matched by the rate at which it is rebuilt. Osteoporosis occurs when this balance shifts in favor of resorption, meaning bone is being broken down faster than it is being rebuilt, and bone mineral density progressively declines (Föger-Samwald et al., 2020).
The most common contributors to this imbalance are estrogen deficiency, particularly in postmenopausal women, and vitamin D deficiency. Estrogen plays a key role in regulating osteoclast activity; after menopause, when estrogen levels decline, osteoclast activity becomes relatively unchecked, accelerating bone resorption. Vitamin D is essential for calcium absorption and utilization, making it a critical cofactor in bone formation.
It is also worth noting that both of the other conditions discussed today, diabetes and thyroid disease, can increase the risk of osteoporosis. The connections are multiple and complex, but one practical takeaway is that a patient with type 1 diabetes, with hypothyroidism, or on long-term levothyroxine at an excessive dose is at elevated risk for bone loss and should be screened accordingly.
Osteoporosis is often called a silent disease because it typically produces no symptoms until a fracture occurs. The most common fracture sites are the hip, the wrist, and the spine. Before a fracture, we might observe height loss of 1 inch or more, or a postural change such as increased thoracic kyphosis, as vertebral compression fractures accumulate over time.
The primary diagnostic tool is a bone density test, commonly called a DEXA (dual-energy X-ray absorptiometry) scan, which measures bone mineral density. Results are reported as a T-score, which reflects the patient's bone mineral density compared to a reference population of young healthy adults.
A T-score of -1.0 or higher is considered normal. A T-score between -1.0 and -2.5 indicates osteopenia, which is decreased bone mineral density that does not yet meet the threshold for osteoporosis. A T-score of -2.5 or lower is diagnostic for osteoporosis. Severe osteoporosis is defined as a T-score of -2.5 or lower combined with one or more fragility fractures.
The FRAX tool (Fracture Risk Assessment Tool) is a supplementary resource that estimates a patient's 10-year probability of hip fracture or major osteoporotic fracture based on clinical risk factors. These include age, sex, BMI, personal and family history of fractures, smoking history, alcohol use, corticosteroid use, and diagnoses such as rheumatoid arthritis. FRAX is available in print and online and does not require a DEXA scan, making it useful for initial risk stratification in clinical settings where imaging may not be immediately accessible.
Treatment for Osteoporosis
Non-pharmacological management of osteoporosis is an area where we, as physical and occupational therapists, have a particularly direct and meaningful role. The goals are to reduce fracture risk, minimize ongoing bone loss, prevent disability, and manage pain.
Fall prevention is the most immediate priority. A fragility fracture in a patient with osteoporosis is not simply a bone injury; it is a potentially life-altering event, particularly hip fractures, which carry significant morbidity and mortality risk. Fall prevention programs should assess and address balance, lower extremity strength, vision, hearing, vestibular function, environmental hazards, and fall-risk medications. Any of these factors can contribute to a fall, and addressing them together produces better outcomes than addressing them in isolation.
Weight-bearing exercise is the pharmacological complement to bone-building. Wolff's Law states that bone adapts to the mechanical loads placed upon it. A bone regularly stressed by weight-bearing activity becomes denser and stronger in response to that stress. Walking, Tai chi, yoga, and Pilates are all examples of weight-bearing activities that apply bone-stimulating loads without requiring high impact. For patients who are deconditioned, even a modest, progressively graduated walking program can initiate the activation of this adaptive response.
Education regarding lifestyle factors is also within our scope. That includes vitamin D and calcium intake (≥ 800 IU vitamin D + 700-1200 mg/day of calcium), smoking cessation, and moderation of alcohol intake, which are all modifiable risk factors for osteoporosis progression.
Antiresorptive Medications
Bisphosphonates
The bisphosphonates are the most commonly prescribed first-line pharmacological treatment for osteoporosis.
This class includes:
- Alendronate (Fosamax),
- Risedronate (Actonel),
- Ibandronate (Boniva),
- Zoledronic acid (Reclast).
The anti-resorptive medication denosumab (Prolia), although not a bisphosphonate, is included in this category because it also targets osteoclast activity through a different mechanism.
Bisphosphonates work by impairing osteoclast function, slowing the rate of bone resorption, and thereby allowing the osteoblast-driven bone formation process to gain relative ground. The result over time is maintenance or improvement of bone mineral density.
The administration details of bisphosphonates are clinically important and worth knowing for patient education. Alendronate (Fosamax) and risedronate (Actonel) are commonly prescribed as weekly oral doses, taken after an overnight fast, at least 30 minutes before any food, drink, or other medication, with a full glass of water. The patient must remain upright (sitting or standing) for at least 30 minutes after taking the medication to reduce the risk of esophageal irritation, a GI side effect associated with this class. Ibandronate (Boniva) is available as a monthly pill or as a quarterly infusion. Zoledronic acid (Reclast) is an annual intravenous infusion, which significantly reduces adherence challenges.
Denosumab (Prolia) is a monoclonal antibody that works differently from bisphosphonates. Rather than directly impairing osteoclasts, it targets the signaling protein RANK ligand, which is required for osteoclast generation, thereby reducing osteoclast formation and activity through an immune-mediated mechanism. It is administered by subcutaneous injection every six months.
Important side effects to be aware of across this class include GI symptoms, osteonecrosis of the jaw (a rare but serious adverse effect involving bone death in the jaw that can be associated with dental procedures in patients on long-term bisphosphonates), and atypical femur fractures (Chandran et al., 2024). The atypical femur fractures associated with bisphosphonate use are a particularly important concern for therapists. These fractures typically occur in the subtrochanteric or femoral shaft region and may be heralded by prodromal thigh or groin pain. In any patient on a bisphosphonate who reports new-onset hip or thigh pain without a clear traumatic mechanism, this should be communicated to the medical team promptly.
Selective estrogen receptor modulators, or SERMs, such as raloxifene (Evista), mimic the bone-protective effects of estrogen in bone tissue while avoiding estrogen-related risks in other tissues, such as the breast or uterus. They are another option in the anti-resorptive category, particularly for postmenopausal women for whom bisphosphonates may not be appropriate.
Anabolic Medications
While anti-resorptive medications focus on slowing bone breakdown, anabolic medications stimulate bone formation. Examples include teriparatide (Forteo) and abaloparatide (Tymlos). These medications function as parathyroid hormone analogs.
The parathyroid glands, which sit on the posterior surface of each thyroid lobe, produce parathyroid hormone (PTH), which regulates calcium homeostasis. In its intermittent, pulsatile form, parathyroid hormone promotes bone formation; when chronically elevated, it promotes resorption. Teriparatide and abaloparatide exploit the bone-forming effects of intermittent PTH exposure to stimulate osteoblast activity and increase bone mass.
Side effects can include GI disturbance and joint, leg, or back pain. There is a black box warning for this class regarding the risk of osteosarcoma (bone cancer), which has been observed in animal models at high doses. This warning also includes concerns about hypercalcemia. These medications are generally reserved for patients with severe osteoporosis or those who have not responded adequately to anti-resorptive therapy.
Combination Medications
The newest category in osteoporosis pharmacology is the combination agent, represented by romosozumab (Evenity). This monoclonal antibody works through a dual mechanism: it simultaneously stimulates bone formation and inhibits bone resorption. By addressing both ends of the remodeling imbalance at once, it produces changes in bone mineral density that are more rapid and pronounced than either class alone.
Romosozumab carries a black box warning for increased cardiovascular risk, including heart attack, stroke, and cardiovascular death. Its FDA approval came after regulatory delays related to these cardiovascular concerns, and it is used selectively in patients in whom the benefits of rapid bone density improvement outweigh the cardiovascular risks.
Therapy Implications
Our contributions to osteoporosis management are substantial, and we should approach them with intention. The foundational strategies align with what I have already described: fall reduction through balance and strengthening interventions, promotion of weight-bearing exercise to invoke Wolff's Law, and patient education regarding lifestyle factors.
From a pharmacological standpoint, the most important therapy-specific consideration is awareness of the side effects that have direct clinical relevance. For patients on bisphosphonates, we should be alert to new hip or thigh pain. Atypical femur fractures can present as insidious-onset pain in the subtrochanteric region before any fracture has occurred on imaging. If a patient on Fosamax or another bisphosphonate reports new or worsening thigh pain, this warrants communication with the prescriber.
We should also be familiar with the specific administration requirements for bisphosphonates, particularly the upright positioning requirement for oral forms. If a patient is on Fosamax and has difficulty maintaining upright sitting or standing for 30 minutes after morning medications due to their mobility limitations, this is a clinically relevant piece of information to discuss with them and, when appropriate, to flag with the medical team.
Finally, for patients on anabolic medications, awareness of the symptoms of hypercalcemia (nausea, fatigue, bone pain, confusion, increased thirst and urination) is worth having, as this is a known risk of parathyroid hormone analogs.
Case Studies
Case Study – Mrs. D
Mrs. D is a 65-year-old woman with a medical history of type 2 diabetes and hypothyroidism who presents to outpatient physical therapy for shoulder pain. Her current medications include metformin, Victoza (liraglutide), and levothyroxine.
Let me walk through what each of those medications tells us about her management and the considerations that belong in our clinical thinking.
Metformin, as the only biguanide, is likely her foundational diabetes medication, probably one of the first she was prescribed. It reduces hepatic glucose production and poses a low risk of hypoglycemia. We would not expect her metformin to create hypoglycemia risk during a shoulder rehabilitation session under typical circumstances.
Victoza is the brand name for liraglutide, a GLP-1 receptor agonist. Its presence on her list means she is receiving incretin-mimetic therapy in addition to her metformin, addressing her hyperglycemia through a second mechanism: slowing gastric emptying, stimulating insulin release in a glucose-dependent manner, and inhibiting glucagon. The combination of metformin and a GLP-1 agonist is a common pairing in type 2 diabetes management, reflecting the polypharmacy strategy I described earlier: two different mechanisms, two different targets, and lower doses of each. Because GLP-1 receptor agonists do not directly drive hypoglycemia (their insulin-stimulating effect is glucose-dependent), her hypoglycemia risk from these two medications alone is relatively low. However, if she were to experience nausea or any GI side effects from the Victoza, particularly if her dose has been recently adjusted, this may affect her participation in therapy.
Levothyroxine tells us that her hypothyroidism has been diagnosed and is being treated. Our monitoring role is to watch for signs that the pendulum has swung too far: tachycardia, diaphoresis beyond what exercise warrants, tremor, or agitation could all signal that her dose is producing hyperthyroid effects. Dosing of levothyroxine often requires adjustment over time, and the transition period is when we are most likely to encounter signs of imbalance in either direction.
It is also worth holding in mind the general clinical principle I raised earlier: if the musculoskeletal presentation of a patient with a known or suspected endocrine disorder does not fully match the history or mechanism, consider whether the endocrine condition may be contributing to the symptom picture. Her shoulder pain may have a clear structural etiology, but if the response to treatment is atypical, keeping the hypothyroidism in view as a potential systemic contributor is sound clinical reasoning.
Case Study – Ms. P
Ms. P is a 70-year-old woman with type 1 diabetes and osteoporosis who is receiving home health physical therapy for falls. Her current medications include insulin and alendronate (Fosamax).
The insulin tells us everything we need to know about her type 1 diabetes management: because her autoimmune condition has eliminated her body's capacity to produce insulin, providing exogenous insulin is the only option. She may be on more than one type, for example, a long-acting basal insulin like glargine combined with ultra-rapid-acting insulin at mealtimes. The specific types, doses, and injection schedule should be clarified, as they directly affect our clinical planning.
Her primary therapy concern from an insulin standpoint is hypoglycemia risk, and for Ms. P, this risk is compounded in a way that deserves deliberate attention. We are seeing her in home health for falls, and our plan almost certainly involves increasing her activity through strengthening, balance training, and weight-bearing exercise, which is appropriate and important for both her fall risk and her osteoporosis. But every increase in weight-bearing, large-muscle-group activity activates the insulin-independent GLUT4 uptake pathway. If her insulin regimen is not adjusted to account for this additional glucose-lowering mechanism, she is at elevated risk for hypoglycemia not only during our sessions but for up to 72 hours afterward.
The conversation with her and her medical team should include the importance of monitoring blood glucose before, during, and, if possible, after exercise sessions, and the recognition that the insulin-independent effect of exercise on glucose uptake is a real and significant clinical variable. Pre-exercise blood glucose below 100 mg/dL should prompt a snack before activity. Glucose above 300 mg/dL should prompt postponement of the session.
Alendronate (Fosamax) indicates that her osteoporosis is being pharmacologically managed through osteoclast inhibition, slowing bone resorption. Our clinical complement to this medication is to activate Wolff's Law by introducing and progressively increasing weight-bearing activities that stimulate bone formation in response to mechanical loading. Walking, Tai chi, and targeted strength exercises are all appropriate tools.
We should also monitor for the atypical femur fractures associated with bisphosphonate use. Ms. P is being seen for falls, which already places her at elevated fracture risk. If she reports new or worsening hip or thigh pain at any point during our care, this should be taken seriously and communicated to her prescriber. The bisphosphonate is doing important work for her bone density, but the atypical fracture risk is a known trade-off that warrants clinical vigilance.
Summary
Over the course of this session, we have covered substantial ground across three endocrine conditions and a broad range of pharmacological agents. I want to close by tying these threads back to the learning outcomes and the core message I carry into every pharmacology course I teach.
Diabetes mellitus, regardless of type, is a state of hyperglycemia. The pharmacological goal in every case is to reduce blood glucose toward the normal range without swinging too far in the other direction into hypoglycemia. As therapists, our most direct contributions are recognizing the signs of hypoglycemia, understanding how exercise amplifies or interacts with insulin's glucose-lowering effects, and educating patients about monitoring and safety. The insulin-independent GLUT4 mechanism is perhaps the most important piece of pharmacology I can offer any therapist who works with patients with diabetes: muscle contraction during aerobic exercise moves glucose transporters to the cell surface, without requiring insulin. Exercise is medicine in the most literal physiological sense.
Hypothyroidism is a condition with a slow, diffuse presentation that can masquerade as musculoskeletal pathology. Clinicians who recognize the symptom pattern of undiagnosed hypothyroidism, particularly swelling of the small joints of the hands and feet, fatigue, cold intolerance, and carpal tunnel without a mechanical explanation, provide real value to their patients. For those on treatment, monitoring for imbalance toward hyperthyroidism as the dose is titrated and implementing aerobic training to help restore activity tolerance are our most practical contributions.
Osteoporosis is a silent disease until it is not. Fall prevention is our most powerful intervention, and it operates across every dimension of our scope of practice: strength, balance, vestibular function, vision, environmental assessment, and medication awareness. Weight-bearing exercise invokes Wolff's Law, the principle that bone responds to mechanical stress by becoming denser and stronger. And familiarity with the side-effect profiles of bisphosphonates, particularly atypical femoral fractures and osteonecrosis of the jaw, makes us better partners in the management of our patients' bone health.
Pharmacology can feel overwhelming. I have spent ten years watching that feeling arise in students and in licensed therapists alike. But when it is taught through the lens of pathophysiology, through the biology of what is going wrong and the logic of what each medication is trying to fix, it becomes manageable. I hope that today you have walked away with something you will use, even if it is just one clinical pearl that changes how you approach a patient next week. Thank you for your time and your commitment to your patients' care.
References
American Diabetes Association. (n.d.). Insulin basics. https://diabetes.org/health-wellness/medication/insulinbasics
American Diabetes Association. (2026). Oral and other injectable diabetes medications. https://diabetes.org/health-wellness/medication/oral-other-injectable-diabetes-medications
Chandran, M., Akesson, K. E., Javaid, M. K., et al. (2024). Impact of osteoporosis and osteoporosis medications on fracture healing: A narrative review. Osteoporosis International, 35, 1337–1358. https://doi.org/10.1007/s00198-024-07059-8
Cleveland Clinic. (2026). GLP-1 agonists. https://my.clevelandclinic.org/health/treatments/13901-glp1-agonists
Colberg, S. R., Sigal, R. J., Fernhall, B., et al. (2010). Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care, 33(12), e147–e167.
Colberg, S. R., Sigal, R. J., Yardley, J. E., et al. (2016). Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care, 39, 2065–2079.
Cuff, D. J., Meneilly, G. S., Martin, A., Ignaszewski, A., Tildesley, H. D., & Frohlich, J. J. (2003). Effective exercise modality to reduce insulin resistance in women with type 2 diabetes. Diabetes Care, 26(11), 2977–2982.
Davis, M. G., & Phillippi, J. C. (2022). Hypothyroidism: Diagnosis and evidence-based treatment. Journal of Midwifery & Women's Health, 67, 394–397. https://doi.org/10.1111/jmwh.13358
Drucker, D. J. (2024). Efficacy and safety of GLP-1 medicines for type 2 diabetes and obesity. Diabetes Care, 47(11), 1873–1888. https://doi.org/10.2337/dci24-0003
Föger-Samwald, U., Dovjak, P., Azizi-Semrad, U., Kerschan-Schindl, K., & Pietschmann, P. (2020). Osteoporosis: Pathophysiology and therapeutic options. EXCLI Journal, 19, 1017–1037. https://doi.org/10.17179/excli2020-2591
Holst, J. J. (2022). Glucagon-like peptide-1: Are its roles as endogenous hormone and therapeutic wizard congruent? Journal of Internal Medicine, 291, 557–573.
Mayo Clinic. (2026). Hypothyroidism. https://www.mayoclinic.org/diseases-conditions/hypothyroidism/expertanswers/hypothyroidism/faq-20057789
McCulloch, D. K. (2018a). Effects of exercise in adults with diabetes mellitus. UpToDate. https://www.uptodate.com/contents/effects-of-exercise-in-adults-with-diabetes-mellitus
McCulloch, D. K. (2018b). General principles of insulin therapy in diabetes mellitus. UpToDate. https://www.uptodate.com/contents/general-principles-of-insulin-therapy-in-diabetes-mellitus
Messina, G., Alioto, A., Parisi, M. C., Mingrino, O., Di Corrado, D., Crescimanno, C., Kuliś, S., Nese Sahin, F., Padua, E., Canzone, A., & Francavilla, V. C. (2023). Experimental study on physical exercise in diabetes: Pathophysiology and therapeutic effects. European Journal of Translational Myology, 33(4), 11560. https://doi.org/10.4081/ejtm.2023.11560
National Institute of Diabetes and Digestive and Kidney Diseases. (2026a). Hypothyroidism. https://www.niddk.nih.gov/health-information/endocrine-diseases/hypothyroidism
National Institute of Diabetes and Digestive and Kidney Diseases. (2026b). Prescription medications to treat overweight & obesity. https://www.niddk.nih.gov/health-information/weight-management/prescription-medications-treat-overweight-obesity
Navale, A. M., & Paranjape, A. N. (2016). Glucose transporters: Physiological and pathological roles. Biophysical Reviews, 8(1), 5–9.
Ojo, O. A., Ibrahim, H. S., Rotimi, D. E., Ogunlakin, A. D., & Ojo, A. B. (2023). Diabetes mellitus: From molecular mechanism to pathophysiology and pharmacology. Medicine in Novel Technology and Devices, 19, 100247. https://doi.org/10.1016/j.medntd.2023.100247
Shivaprasad, C., & Kalra, S. (2011). Bromocriptine in type 2 diabetes mellitus. Indian Journal of Endocrinology and Metabolism, 15(Suppl 1), S17–S24. https://doi.org/10.4103/2230-8210.83058
Umpierre, D., Ribeiro, P. A., Kramer, C. K., et al. (2011). Physical activity advice only or structured exercise training and association with HbA1c levels in type 2 diabetes: A systematic review and meta-analysis. JAMA, 305(17), 1790–1799.
Bednarek, M. (2026, May). GLP-1s and More: Pharmacology for Diabetes Mellitus and Other Endocrine Conditions. PhysicalTherapy.com, Article 5023. Retrieved from: https://www.physicaltherapy.com
